Overview of Commonly Used Immunohistochemical Markers for B-Cell Lymphoma
Commonly used immunohistochemical markers in the diagnosis of B-cell lymphoma include: CD5, CD10, CD19, CD20, CD23, CD79a, PAX-5, BCL-2, BCL-6, cyclin D1, SOX-11, ARTA1, TdT.
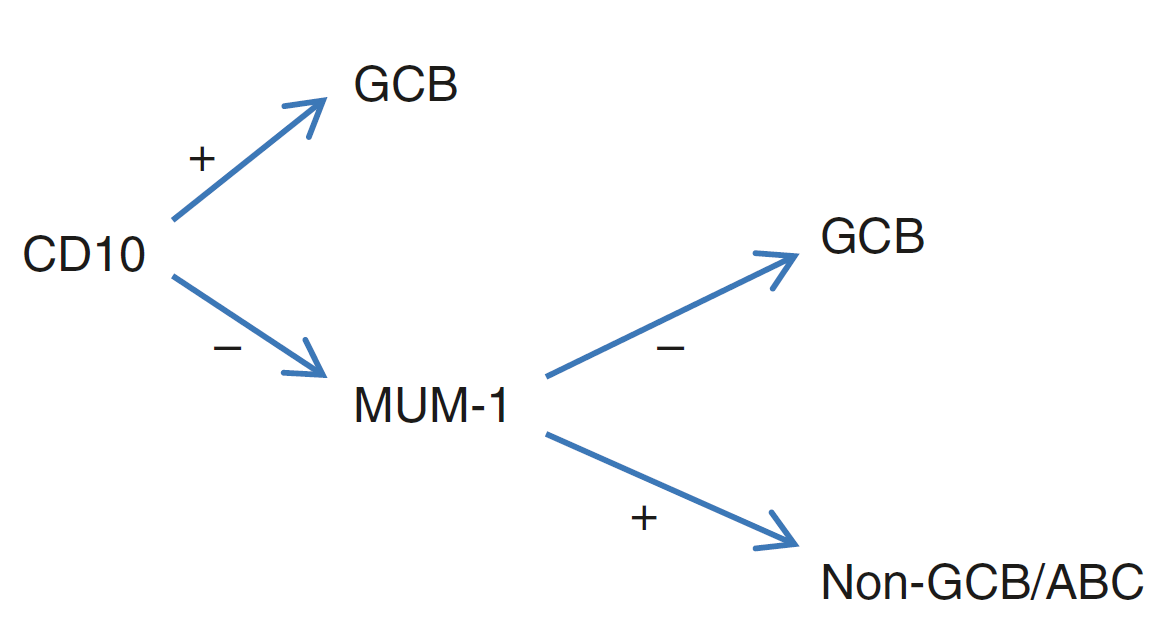
Figure 1. Application of CD10 in Hans classification of diffuse large B-cell lymphoma: CD10 positive, or CD10 negative and MUM-1 negative, consider germinal center B-cell origin; CD10 negative and MUM-1 positive, consider non-germinal center origin, activated B-cell type.
Detailed Explanation of Specific Markers
Positive expression pattern: Cell membrane
Recommended positive control tissue: Appendix/Tonsil
CD19 is an early naive B lymphocyte antigen, present throughout the differentiation stages of B lymphocytes, but disappears at the plasma cell stage. Therefore, this marker is an excellent B lymphocyte marker.
Positive expression pattern: Cell membrane
Recommended positive control tissue: Appendix/Tonsil
CD20 functions as a receptor during B-cell activation and differentiation, expressed after the CD19-positive naive B-cell differentiation stage, and persists in the later stages of B lymphocyte differentiation, but is not expressed at the plasma cell stage.
CD20 is a broad-spectrum B-cell marker, but certain types of B-cell lymphoma are negative or show very weak expression. Therefore, for uncertain cases, it is essential to use two B-cell markers to confirm or exclude the B-cell origin of the tumor. Ideal combinations are CD20+CD19, CD20+PAX-5, or CD20+CD79a.
Generally, CD20 expression is confined to B lymphocytes, but rare cases of peripheral T-cell lymphoma expressing CD20 have been reported. Another diagnostic pitfall is the interpretation of CD20 staining in specimens after CD20-targeted therapy (Rituximab), which requires caution. Nuclear or nucleolar CD20 staining is non-specific.
Positive expression pattern: Cell membrane
Recommended positive control tissue: Appendix/Tonsil
CD23, also known as the low-affinity IgE receptor, is involved in the regulation of IgE effects. This marker is expressed on mature B lymphocytes, follicular dendritic cells, and activated macrophages. Therefore, it is an important marker for distinguishing B-cell chronic lymphocytic leukemia from other lymphomas with similar morphology; it can also be used for the identification of follicular dendritic cell tumors. CD23 can also be expressed in mediastinal large B-cell lymphoma and lymphoplasmacytic lymphoma.
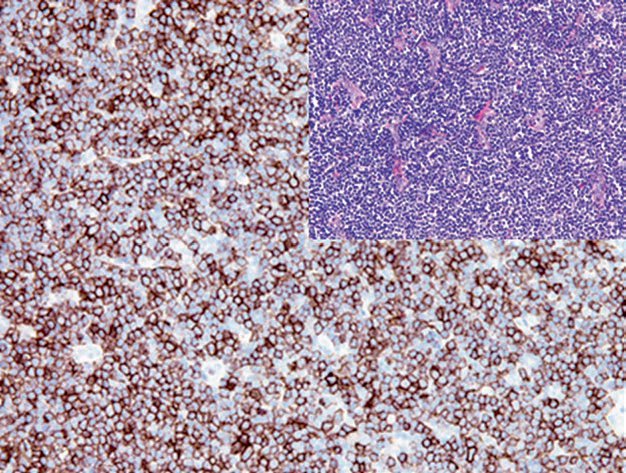
Figure 2. In B-cell chronic lymphocytic leukemia, CD23 shows positive expression on the cell membrane.
Positive expression pattern: Cell membrane
Recommended positive control tissue: Appendix/Tonsil
CD79a appears at the precursor B lymphocyte stage and persists until the plasma cell development stage, so most normal and neoplastic plasma cells also express CD79a. CD79a stains the cell membrane, but cytoplasmic staining can also occur in plasma cells. Meanwhile, CD79a expression is independent of CD20 expression, and CD79a remains positive after anti-CD20 targeted therapy. However, for the diagnosis of B-cell lymphoma, CD79a is less reliable than CD20 because this marker is positive in a small subset of T-lymphoblastic leukemia, acute myeloid leukemia (M3 type), and most plasma cell neoplasms.
Positive expression pattern: Nucleus
Recommended positive control tissue: Appendix/Tonsil
During B-cell development, Pax-5 is expressed from progenitor B cells, precursor B cells, naive B cells to mature B cells. The Pax-5 encoding gene is located at 9p13, so the translocation t(9;14)(p13;q32) associated with the plasma cell subtype in small lymphocytic lymphoma also involves Pax-5. Rarely, it can also be expressed in T-cell-derived acute lymphoblastic lymphoma. Pax-5 can also be expressed in acute myeloid leukemia, mainly related to the t(8;21)(q22;q22) translocation. Additionally, this marker is expressed in the hallmark tumor cells of nodular lymphocyte predominant Hodgkin lymphoma. T lymphocytes, plasma cells, and macrophages are all Pax-5 negative.
Some other tumors resembling lymphoma may have positive Pax-5 expression, such as Merkel cell carcinoma and small cell carcinoma. Rarely, Pax-5 positivity has been reported in breast, endometrial, transitional cell carcinoma, and alveolar rhabdomyosarcoma, but it is negative in embryonal rhabdomyosarcoma.
Positive expression pattern: Nucleus
Recommended positive control tissue: Mantle cell lymphoma
Mantle cell lymphoma has a t(11;14) translocation, leading to cyclin D1 overexpression, which is a characteristic marker of this lymphoma. A small subset of mantle cell lymphomas do not express cyclin D1, but in such cases, they generally express SOX-11, which can aid in differential diagnosis. Some multiple myelomas also have the t(11;14) translocation, resulting in positive cyclin D1 expression, and this situation generally indicates a better prognosis. Other lymphomas with similar morphology can also express cyclin D1, such as hairy cell leukemia and B-cell chronic lymphocytic leukemia; however, the staining intensity is weaker than in mantle cell lymphoma. In routine work, cyclin D1 is generally used in combination with CD5, SOX-11, and other B-cell markers.
Cyclin D1 expression is not limited to lymphoid tumors; it is also seen in a large number of non-lymphoid epithelial tumors and mesenchymal tumors.
Positive expression pattern: Nucleus
Recommended positive control tissue: Mantle cell lymphoma
In mantle cell lymphoma and others such as hairy cell leukemia and acute lymphoblastic leukemia, regardless of cyclin D1 expression results, SOX-11 is strongly positive. This marker can also be expressed in some ovarian cancers, where it generally indicates a good prognosis.
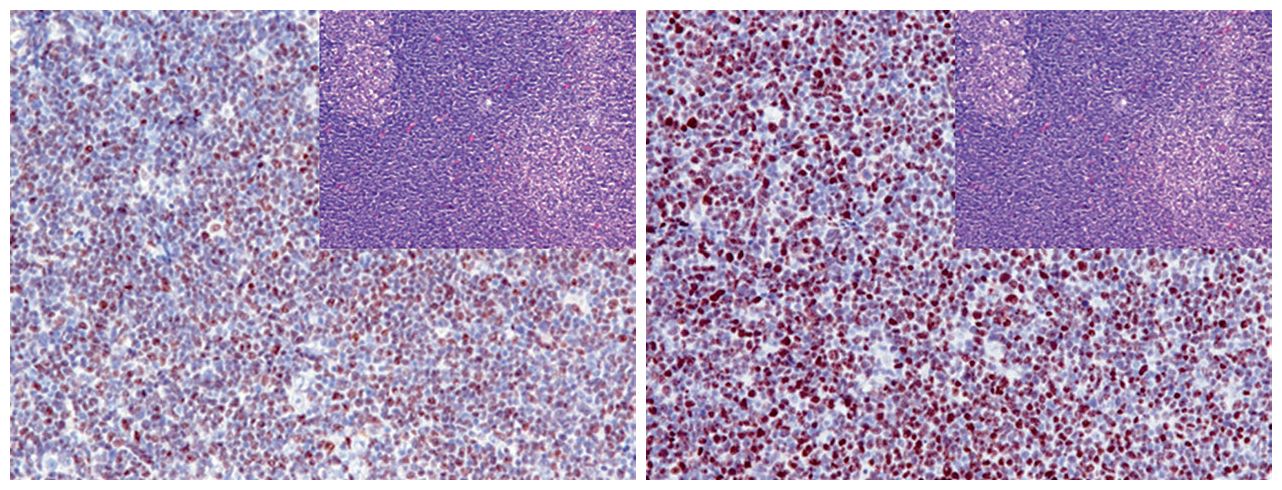
Figure 3. In mantle cell lymphoma, cyclin D1 (left) and SOX-11 (right) show strong positive nuclear expression.
Positive expression pattern: Nucleus
Recommended positive control tissue: Appendix/Tonsil
BCL-6 is expressed in normal germinal center B lymphocytes. Therefore, this marker is a marker for germinal center-derived lymphomas, such as follicular lymphoma (intrafollicular and interfollicular cells), Burkitt lymphoma, most Hodgkin cells, and nodular lymphocyte predominant Hodgkin lymphoma. BCL-6 positivity can also be seen in some NK/T-cell lymphomas, such as angioimmunoblastic lymphoma and acute T-lymphoblastic leukemia. Mantle cell lymphoma and marginal zone lymphoma are BCL-6 negative.
Positive expression pattern: Cytoplasm (and mitochondrial membrane)
Recommended positive control tissue: Appendix/Tonsil
The BCL-2 gene is located at 18q21, transcribing three mRNAs, which then form two homologous essential cellular proteins and mitochondrial membrane proteins. 90% of follicular lymphomas have the t(14;18)(q32;q21) translocation, so the BCL-2 gene combines with the Ig heavy chain gene, leading to BCL-2 protein overexpression, allowing lymphoma cells to survive.
The main use of BCL-2 in diagnosis is to distinguish reactive lymph nodes with follicular hyperplasia (BCL-2 negative) from grade 1 follicular lymphoma (with BCL-2 positive neoplastic B cells within follicles). However, it should be noted that BCL-2 positivity is seen in most B-cell lymphomas and some T-cell lymphomas, and this marker is also positively expressed in a large number of epithelial and mesenchymal tumors.
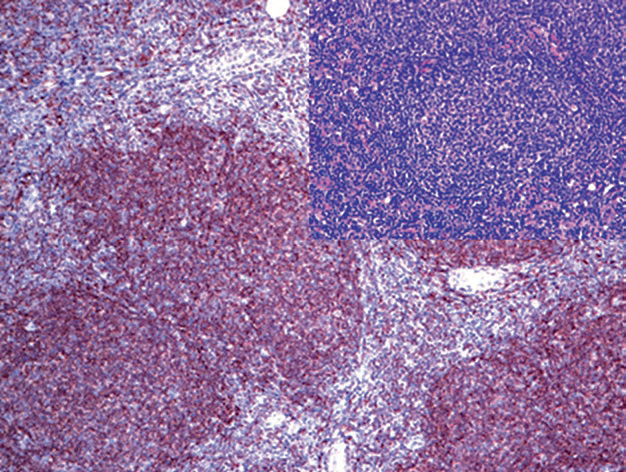
Figure 4. Follicular lymphoma, with diffuse strong positivity for BCL-2 in neoplastic follicles.
Positive expression pattern: Cell membrane
CD11c is mainly expressed in myeloid hematopoietic cells, so this marker is used to distinguish lymphoid tissue tumors from myeloid tumors. It is strongly positive in hairy cell leukemia and NK-cell lymphoma. About 50% of acute myeloid leukemias (M4 and M5), some follicular lymphomas, Langerhans cell histiocytosis, lymphoplasmacytic lymphoma, splenic lymphoma with villous lymphocytes, and B-cell chronic lymphocytic leukemia express CD11c. CD11c positivity in B-cell chronic lymphocytic leukemia is generally associated with a better prognosis.
Positive expression pattern: Cytoplasm
Recommended positive control tissue: Osteoclasts, hairy cell leukemia
Tartrate-resistant acid phosphatase (TRAP) can be expressed in various tissues, with high expression in osteoclasts and macrophages. This marker is specific for hairy cell leukemia but can also be used in combination with other markers, such as CD11c and DBA.44. Weak TRAP expression can also occur in other lymphomas, such as marginal zone B-cell lymphoma; when used for bone marrow specimen evaluation, note that macrophages in the bone marrow are TRAP positive.
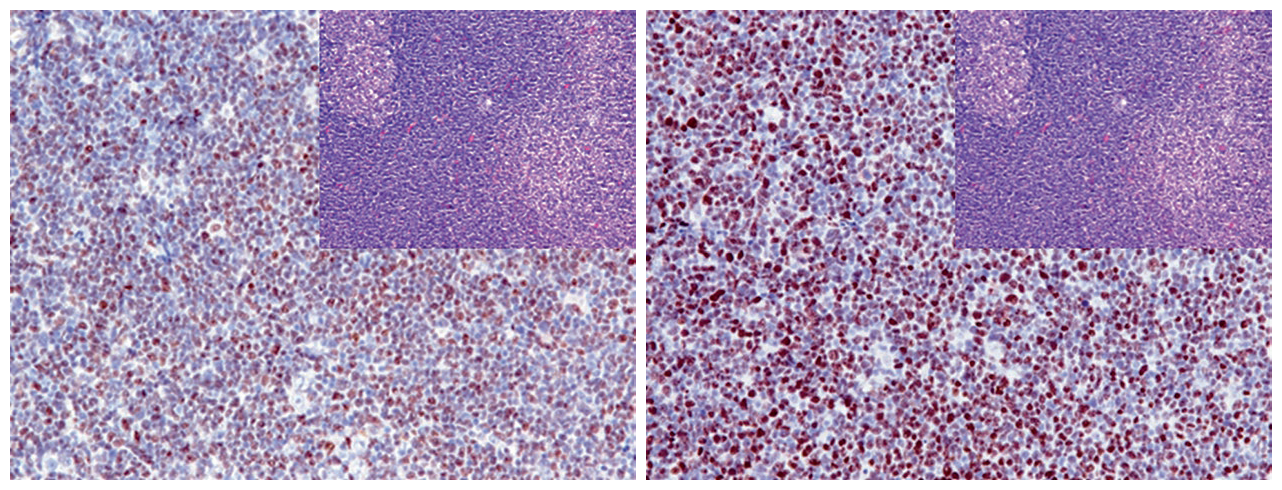
Figure 5. Bone marrow trephine biopsy specimen, showing CD11c positive leukemia cells (left); and TRAP is also strongly positive (right).
Immunoglobulin Superfamily Receptor Translocation-1 (IRTA-1) helps distinguish marginal zone lymphoma from other lymphomas because its positivity rate is over 90% in extranodal marginal zone lymphoma and about 75% in nodal marginal zone lymphoma. Other lymphomas such as B-cell chronic lymphocytic leukemia, mantle cell lymphoma, follicular lymphoma, Burkitt lymphoma, hairy cell leukemia, plasma cell neoplasms, etc., do not express it. However, this marker cannot distinguish whether marginal zone lymphocytes are reactive or neoplastic.
Positive expression pattern: Nucleus
Recommended positive control tissue: Tonsil/Lymph node
LMO-2 is normally expressed in erythroid and myeloid precursors, megakaryocytes, endothelial cells, and also in germinal center B lymphocytes, making it a marker for several germinal center cell-derived lymphomas. For all grades of follicular lymphoma, the LMO-2 positivity rate is 70%; it is also expressed in mediastinal large B-cell lymphoma, Burkitt lymphoma, diffuse large B-cell lymphoma, B-cell and T-cell acute lymphoblastic leukemia. Additionally, myeloblasts in myeloid leukemia express LMO2. Generally, LMO-2 is not expressed in chronic lymphocytic leukemia, mantle cell lymphoma, marginal zone lymphoma, lymphoplasmacytic lymphoma, and peripheral T-cell lymphoma. Besides lymphoid and hematopoietic tumors, LMO2 is expressed in normal endothelial cells of blood and lymphatic vessels, so it is also expressed in most benign and malignant endothelial cell tumors.
Human germinal center-associated lymphoma (HGAL), also known as germinal center B-cell-expressed transcript 2 (GCET-2), is expressed only in the cytoplasm and membrane of germinal center B lymphocytes, with higher expression levels in proliferating cells in the germinal center light zone. It is not expressed in the mantle zone, marginal zone, interfollicular area, or paracortical area. Therefore, HGAL is a marker for germinal center lymphocyte-derived B-cell lymphomas, with a 100% positivity rate in Burkitt lymphoma, over 90% in follicular lymphoma and mediastinal lymphoma, and about 70% in diffuse large B-cell lymphoma. The positivity rate of HGAL in marginal zone lymphoma is less than 5%, while it is completely negative in mantle cell lymphoma and B-cell chronic lymphocytic leukemia.
Lymphoid enhancer-binding factor-1 (LEF-1) is a nuclear protein normally expressed in precursor B cells and precursor T cells, but not in mature B cells. In lymphoma, LEF-1 is expressed in neoplastic small lymphocytes of chronic lymphocytic leukemia but not in other small B-cell lymphomas. Additionally, about one-third of diffuse large B-cell lymphomas express this marker. However, LEF-1 is not a lymphoma-specific marker because it can also be expressed in several carcinomas, such as colorectal adenocarcinoma.
MaiMai Recommendation: “The pathological classification of lymphoma is complex, and its clinical and histological manifestations are ever-changing, making many pathologists sigh at the sight of lymphoma. Immunohistochemistry greatly aids in the diagnosis of lymphoma, and how to use this tool effectively is very important.”
|
Antibody Name
|
Clone Number
|
Positive Control
|
Cellular Localization
|
|
Bcl-2*
|
MX022
|
Tonsil, Appendix
|
CytoplasmMembrane/Cytoplasm
|
|
Bcl-6*
|
MX042
|
Tonsil, Appendix
|
Nucleus
|
|
CD19*
|
MX016
|
Tonsil, Appendix
|
CytoplasmMembrane
|
|
CD20*
|
MX002
|
Tonsil, Appendix
|
Cell Membrane
|
|
CD23
|
SP23
|
Tonsil, Appendix |
Cell Membrane
|
|
CD79a*
|
MX076
|
Tonsil, Appendix
|
Cell Membrane
|
|
Cyclin D1
|
SP4
|
Tonsil |
Nucleus
|
|
LEF-1
|
EP310
|
Tonsil, Appendix
|
Nucleus
|
|
LMO-2
|
SP51
|
Tonsil, Appendix |
Nucleus
|
|
Pax-5*
|
MX017
|
Tonsil, Appendix
|
Nucleus
|
|
SOX-11
|
MRQ58
|
Mantle Cell Lymphoma |
Nucleus
|
*Marked as Maxin clone product
For more information, please contact: 800-8581156 or 400-889-9853
