Overview of Immunohistochemistry in the Diagnosis of Lymphoid Tissue Tumors
Lymphoid tissue is a microenvironment composed of B lymphocytes, T lymphocytes, and NK lymphocytes at different stages of maturation, and also includes plasma cells, histiocytes, dendritic cells, reticular cells, granulocytes, etc., at various differentiation stages. For the diagnosis of lymphoma, all the above components may need to be considered.
In the diagnosis of lymphoma, preliminary screening using certain markers is very helpful; more specific markers are mainly used for more precise diagnosis. The markers and related knowledge introduced in this chapter are also primarily oriented towards diagnostic purposes. The final diagnosis must be a comprehensive judgment based on histomorphology, immunophenotype (immunohistochemistry and flow cytometry), and genetic analysis. It should be noted that the classification of lymphomas considered in this article follows the relevant scheme from the 2016 revision of the World Health Organization classification of lymphoid tissue tumors.
Overview of Commonly Used Markers for Initial Screening of Lymphoma
As mentioned earlier, the composition of lymphoid tissue is very complex; depending on the composition of the lesion, commonly used markers for initial screening of lymphoma generally include: CD45 (LCA), TdT, B-cell markers, T-cell markers, Ki-67. CD5 and CD10 can be used for the diagnosis and further classification of lymphoma, but neither has lineage specificity; they can show positive expression in both B-cell lymphomas and T-cell lymphomas, and can also be expressed in other non-lymphocytic tumors.
Detailed Explanation of Some Markers
Positive Expression Pattern: Cell Membrane
Recommended Positive Control Tissue: Appendix
CD45, also known as leukocyte common antigen (LCA), is expressed in all hematopoietic and blood cells except mature red blood cells and their direct precursor cells, megakaryocytes, and platelets; therefore, this marker is a specific marker for hematopoietic system tumors and lymphoid tumors. However, approximately less than 3% of B-cell lymphomas, about 30% of precursor B-cell lymphomas, and T-lymphoblastic lymphomas (or acute lymphoblastic leukemia) do not express CD45. Therefore, for suspicious cases, other lymph-related markers should be added.
It should be noted that in extremely rare cases, undifferentiated carcinoma, neuroendocrine carcinoma, and small cell carcinoma may show positive cell membrane expression of CD45. Necrotic carcinoma tissue can also show cell membrane staining with this marker; of course, other markers may also show similar situations in necrotic carcinoma tissue, which is a well-known type of false positive.
Positive Expression Pattern: Cell Nucleus
Recommended Positive Control Tissue: T-Lymphoblastic Lymphoma
TdT is a nuclear DNA polymerase, mainly expressed in B-lymphocyte precursors and T-lymphocyte precursors; therefore, this antibody is a specific marker for precursor cell lymphomas of B-cell and T-cell origin, i.e., a specific marker for acute lymphoblastic leukemia.
It should be noted that the proportion of TdT positivity is high in Merkel cell carcinoma, and this tumor can also express Pax-5.
Positive Expression Pattern: Cell Membrane/Cytoplasm
Recommended Positive Control Tissue: Appendix/Tonsil
Although CD10 belongs to the Cluster of Differentiation (CD) series by name, it is a zinc-dependent cell membrane metalloproteinase involved in the processing of neuropeptides and vasoactive peptides after secretion, and has no cell lineage specificity or tumor specificity; therefore, it can be expressed in various tissues such as lymphocytes, epithelial cells, and stromal cells, and related tumors. It should also be noted that depending on the tumor type, the positive expression pattern of CD10 (cell membrane or cytoplasm) varies greatly, but it is not related to tumor grade; cytoplasmic expression is generally seen in poorly differentiated carcinomas.
Positive Expression Pattern: Cell Membrane
Recommended Positive Control Tissue: Appendix/Tonsil
CD5, also known as lymphocyte antigen T1 (Leu-1), is a glycoprotein receptor expressed in most T lymphocytes and some B lymphocytes (including marginal zone lymphocytes); this marker is expressed in various T-cell tumors, such as precursor T-lymphoblastic leukemia, adult and peripheral T-cell lymphoma, mycosis fungoides, and T-cell large granular lymphocytic leukemia. As mentioned earlier, CD5 expression is not limited to T lymphocytes but can also be seen in a minority of B lymphocytes and B-cell-derived lymphomas, the latter mainly including mantle cell lymphoma and B-cell chronic lymphocytic leukemia.
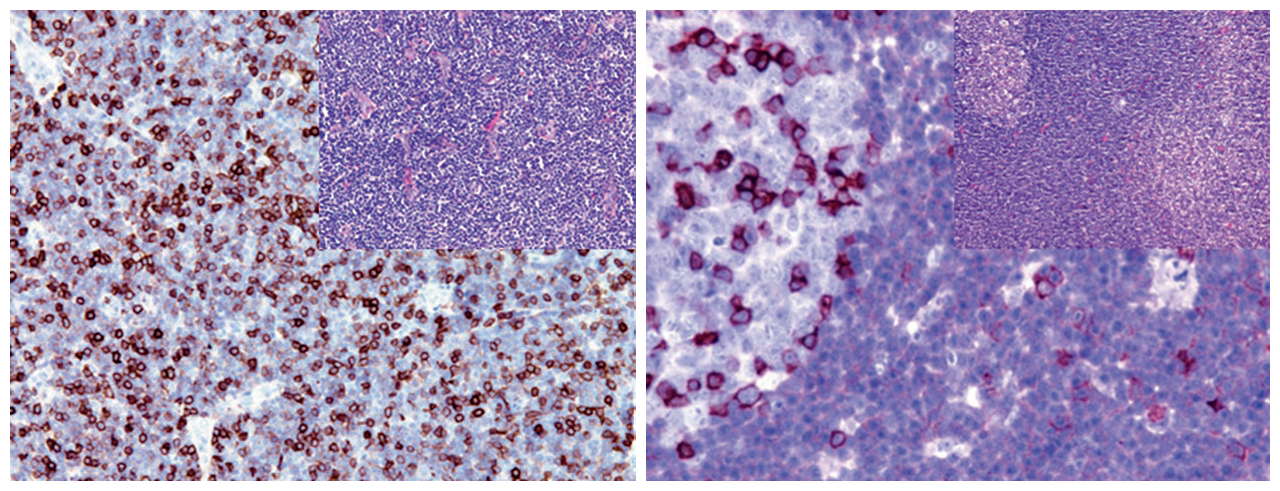
Figure 1. (Left) B-cell chronic lymphocytic leukemia, CD5 shows weak to moderate expression; (Right) Mantle cell lymphoma, CD5 shows moderate cell membrane expression. The strongly positive cells in the figure are T lymphocytes.
CD5 expression is also not limited to lymphoid tissue; it can be expressed in adenocarcinomas of various origins, renal cell carcinoma, adrenocortical carcinoma, and squamous cell carcinoma. In mesothelioma, transitional cell carcinoma, squamous cell carcinoma, and adenocarcinomas of various origins, this marker may show focal weak positive expression; in addition, this marker is also a diagnostic marker for atypical thymoma and thymic carcinoma.
Ki-67 is expressed during the active phase of cell division, specifically starting in the G1 phase, continuing through the S, G2, and M phases, with peak expression occurring in the early M phase, and rapidly degraded at the end of the M phase, with a half-life of 1-1.5 hours. It is not detectable in the G0 phase or the initial stage of the G1 phase. There is no Ki-67 expression during DNA repair.
In routine work, Ki-67 is used to assess cell proliferation, and its positivity level is closely related to cell proliferation activity and tumor grade. At the same time, the Ki-67 proliferation index is also a very important indicator for distinguishing between benign, intermediate, malignant, or low-grade and high-grade tumors. Additionally, it can be used to differentiate atrophy, thermal injury, and dysplasia.
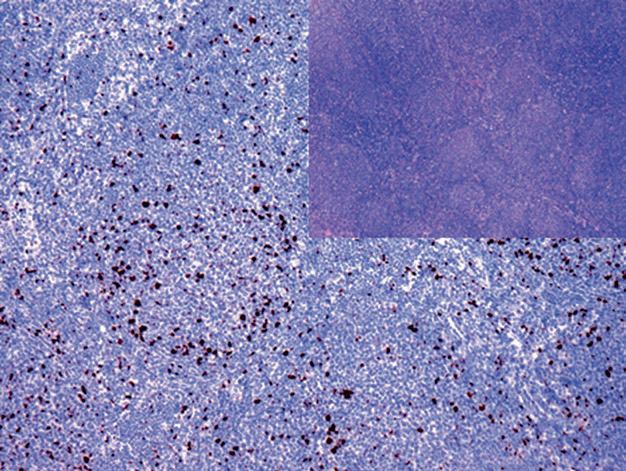
Figure 2. In grade 1-2 follicular lymphoma, the proliferation index of neoplastic follicles is low.
In a few tumors, the Ki-67 proliferation index is almost 100%, specifically such as small cell carcinoma of the lung, Burkitt lymphoma, and plasmablastic lymphoma, which is also one of the diagnostic clues for these tumors. In routine hematopathology work, the Ki-67 proliferation index is an important indicator for distinguishing between low-grade and high-grade lymphomas. Furthermore, the Ki-67 proliferation index is an important prognostic indicator for distinguishing tumor biological behavior, such as in breast cancer and neuroendocrine tumors.
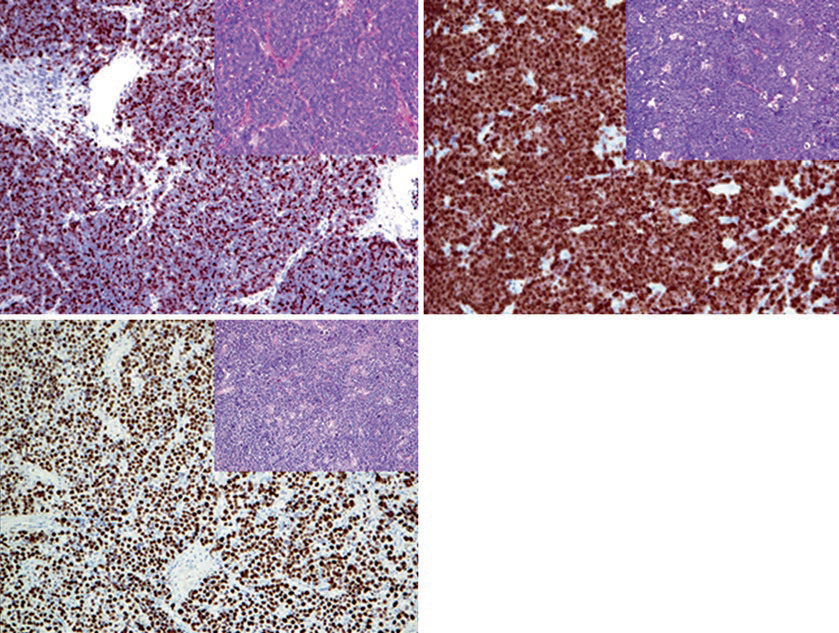
Figure 3. Tumor types with Ki-67 proliferation index close to 100%: (Top left) Small cell carcinoma of the lung; (Top right) Burkitt lymphoma; (Bottom left) Plasmablastic lymphoma.
However, Ki-67 immunohistochemical staining and evaluation still lack standardization, resulting in considerable inter-observer variability, which significantly hinders its clinical application.
MaiMai Recommendation: “Due to space limitations, we will systematically organize and introduce immunohistochemical markers for the diagnosis of lymphoid tissue tumors in multiple installments. Stay tuned. In this issue, MaiMai recommends the following antibodies for you to try.””
|
Antibody Name
|
Clone Number
|
Positive Control
|
Cellular Localization
|
|
CD5*
|
MX052
|
Tonsil, Thymus
|
CytoplasmMembrane
|
|
CD10*
|
MX002
|
Tonsil, Kidney
|
Cytoplasm/Membrane
|
|
CD45
|
PD7/26+2B11
|
Tonsil, Appendix |
Membrane
|
|
TDT*
|
MX010
|
Thymoma
|
Nucleus
|
|
Ki-67*
|
MXR002
|
Tonsil, Breast Cancer |
Nucleus
|
|
Ki-67*
|
MX006
|
Tonsil, Breast Cancer
|
Nucleus
|
*Marked as Maixin clone product
For more information, please contact: 800-8581156 or 400-889-9853
