Overview of Commonly Used Immunohistochemical Indicators for Hodgkin Lymphoma
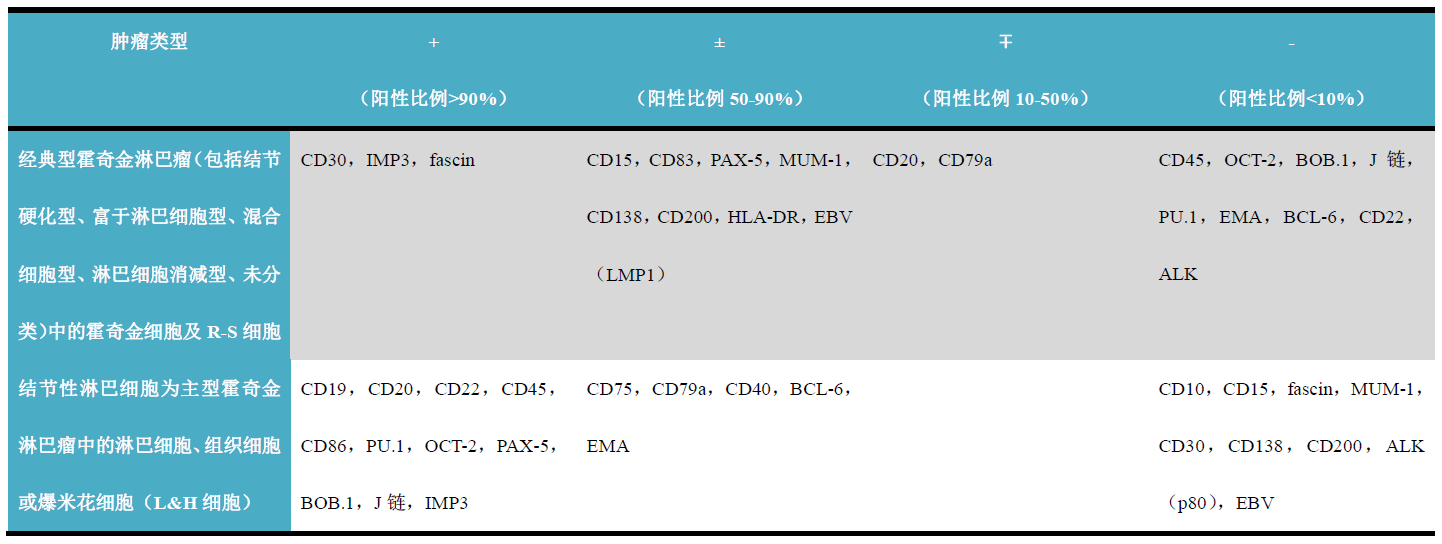
Depending on histological manifestations, Hodgkin lymphoma has various subtypes, with specific classification schemes differing. Overall, commonly used immunohistochemical indicators for diagnosing classical Hodgkin lymphoma include CD15, CD30, MUM-1, IMP3, fascin, and J chain; for nodular lymphocyte-predominant Hodgkin lymphoma, commonly used immunohistochemical indicators include CD19, CD20, PAX-5, J chain, BOB.1, OCT-2, and EMA.
Table 1. Overview of Commonly Used Immunohistochemical Indicators for Hodgkin Lymphoma
Detailed Explanation of Specific Indicators
Positive Expression Pattern: Cell Membrane/Cytoplasm
Recommended Positive Control Tissue: Appendix
CD15 is a cell surface glycoprotein involved in the regulation of neutrophil function, generally used as a marker for normal and neoplastic myeloid cells and monocytes. CD15 is often used in combination with CD30 to mark Reed-Sternberg cells in classical Hodgkin lymphoma.
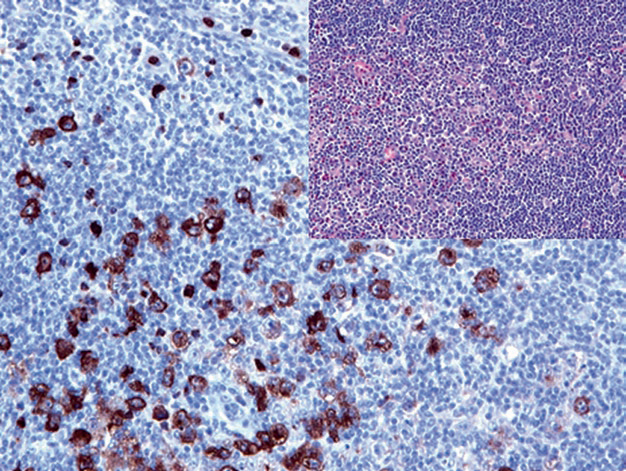
Figure 1. In classical Hodgkin lymphoma, Hodgkin cells are positive for CD15.
It should be noted that CD15 is also expressed in various other hematopoietic system tumors and non-hematopoietic system tumors, such as adenocarcinoma, which should be considered during differential diagnosis; however, mesothelioma is always negative. According to reports, carcinomas positive for CD15 have a poor prognosis.
Positive Expression Pattern: Cell Membrane/Cytoplasm, Perinuclear
Recommended Positive Control Tissue: Embryonal Carcinoma
CD30 is a transmembrane glycoprotein receptor, belonging to the tumor necrosis factor superfamily, involved in the regulation of cell transformation, antibody response, and apoptosis. Normally, CD30 is expressed on activated B cells, T cells, and NK cells. In routine immunohistochemistry, one of the main roles of CD30 is to demonstrate Hodgkin cells and multinucleated Reed-Sternberg cells in classical Hodgkin lymphoma. CD30 is also a diagnostic marker for anaplastic large cell lymphoma, primary mediastinal large B-cell lymphoma, and high-grade types of systemic mastocytosis.
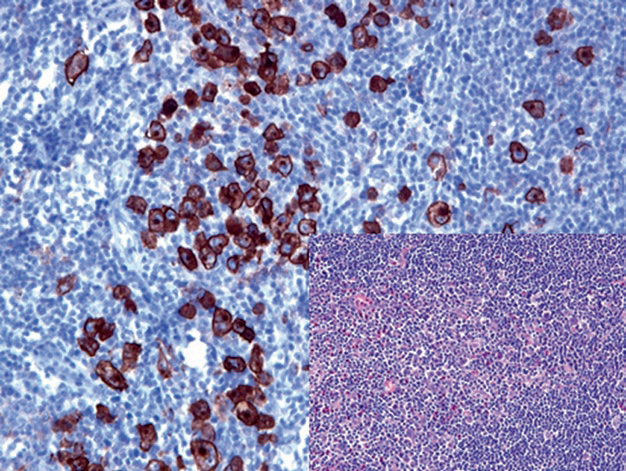
Figure 2. In classical Hodgkin lymphoma, Hodgkin cells are positive for CD30.
It should be noted that CD30-positive cells can be seen in various types of T-cell lymphomas and B-cell lymphomas. CD30 can also mark activated T cells and B cells in reactive lymph nodes, spleen, thymus, and tonsils; therefore, not all CD30-positive cells are Hodgkin cells.
Additionally, CD30 expression is not limited to lymphoid tissues and lymphoid neoplasms; it can also be seen in other epithelial tumors and mesenchymal tumors. CD30 can be used in the diagnosis of embryonal carcinoma; other carcinomas positive for CD30 include nasopharyngeal carcinoma and pancreatic carcinoma. For mesenchymal tumors, approximately 30% of angiosarcomas are CD30 positive.
Positive Expression Pattern: Cell Membrane/Cytoplasm
Recommended Positive Control Tissue: Lymph Node
Fascin is an actin-binding protein involved in cell adhesion and motility. Normally, Fascin is expressed in interdigitating dendritic cells and follicular dendritic cells, variably expressed in endothelial cells, but lymphocytes, plasma cells, and myeloid cells are negative. It is a good marker for Reed-Sternberg cells in classical Hodgkin lymphoma. Additionally, this marker is expressed on the cell membrane in anaplastic large cell lymphoma and in some different types of large B-cell lymphomas.
In normal epithelium, Fascin is generally negative, but it is positive in many transformed or neoplastic epithelia. This phenomenon can be used to differentiate between hyperplastic urothelium and neoplastic urothelium.
Due to the broad expression spectrum of Fascin, careful interpretation of related immunohistochemical results is necessary when used for differential diagnosis. Besides Reed-Sternberg cells, Fascin-positive cells in lymph nodes may also be activated B lymphocytes, cells of diffuse large B-cell lymphoma, or even disseminated metastatic adenocarcinoma cells.
IMP3 is a cytoplasmic protein that mediates RNA exchange and cell growth, highly expressed in early embryonic development. Benign adult tissues generally do not express IMP3, except for fibroblasts, some lymphocytes (mainly germinal center lymphocytes), ovarian and testicular tissues, placenta, and brain. IMP3 is expressed in various precancerous and malignant lesions; carcinomas positive for this marker include lung cancer, esophageal cancer, pancreatic cancer, cervical cancer, endometrial cancer, transitional cell carcinoma, renal cell carcinoma, and neuroendocrine carcinoma. In daily work, IMP3 is used to differentiate malignant lesions from reactive hyperplasia, such as pancreatic cancer being positive while inflammatory pancreatic lesions are generally negative. IMP3 is partially expressed in Hodgkin cells and Reed-Sternberg cells in classical Hodgkin lymphoma and nodular lymphocyte-predominant Hodgkin lymphoma.
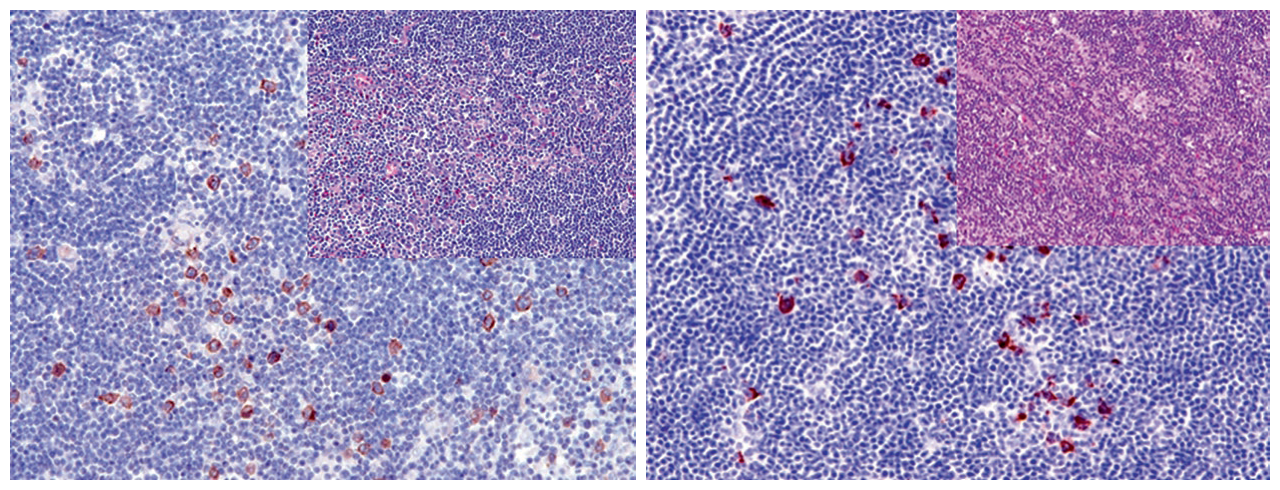
Figure 3. (Left) In classical Hodgkin lymphoma, IMP3 labels some Hodgkin cells; (Right) In nodular lymphocyte-predominant Hodgkin lymphoma, IMP3 labels some Hodgkin cells.
It should be noted that parafollicular blasts may be IMP3 positive, and in such cases, it is necessary to combine other more specific markers to label Hodgkin cells.
MaiMai Recommendation:”Through the above text, I believe many teachers have already memorized the commonly used immunohistochemical indicators for Hodgkin lymphoma and their expression and localization in tissues.However, a successful diagnosis cannot be achieved without a reliable and high-performance antibody.In this issue, MaiMai recommends the following antibodies for you to try.”
|
Antibody Name
|
Clone Number
|
Positive Control
|
Cellular Localization
|
|
CD15
|
MMA
|
Hodgkin Lymphoma, Tonsil
|
Cell Membrane/Cytoplasm
|
|
CD30*
|
MX080
|
Hodgkin Lymphoma, Embryonal Carcinoma
|
CellMembrane/Cytoplasm
|
|
IMP3
|
EP286
|
Pancreatic Cancer, Colon Adenocarcinoma
|
Cell Membrane/Cytoplasm
|
*Marked as Maxin Clone Product
For more information, please contact: 800-8581156 or 400-889-9853
