Overview of Immunohistochemistry for Peritoneal Tumor Diagnosis
For peritoneal tumor diagnosis, the primary issue is selecting appropriate markers based on different morphological considerations. Specifically, commonly used immunohistochemical markers for mesothelial tumors include calretinin, thrombomodulin (CD141), mesothelin, podoplanin (D2-40), WT-1, GLUT-1, BAP-1, h-caldesmon, CD146, and certain CKs; commonly used immunohistochemical markers for Müllerian-derived epithelial tumors include some CKs, CEA, CA125, Pax-8, WT-1, p53, p16; commonly used immunohistochemical markers for smooth muscle tumors are Actin, h-caldesmon, calponin, and some CKs; commonly used immunohistochemical markers for peritoneal primary tumors of unknown origin and other types may involve CD34, CD99, DOG-1, Actin, h-caldesmon, Desmin, ALK, and certain CKs.
Table 1. Overview of Immunohistochemistry for Peritoneal Tumor Diagnosis

(Click to view larger image)
Although peritoneal tumors are diverse, the most critical remains mesothelioma. For the diagnosis of mesothelioma, it is first essential to recognize that mesothelioma does not have a uniform morphological appearance; it can present as epithelioid, sarcomatoid, desmoplastic, or biphasic, and its immunohistochemical phenotype also has many variations. In practical work, it is also important to add other relatively specific markers to exclude other tumors, such as TTF-1, CDX-2, CEA, ER/PR, CD15, etc., which are all negative in mesothelioma. Secondly, distinguishing between benign and malignant mesothelial lesions is crucial, and some immunohistochemical markers are very helpful in this regard.
Table 2. Overview of Immunohistochemical Markers for Differentiating Benign and Malignant Mesothelial Hyperplasia
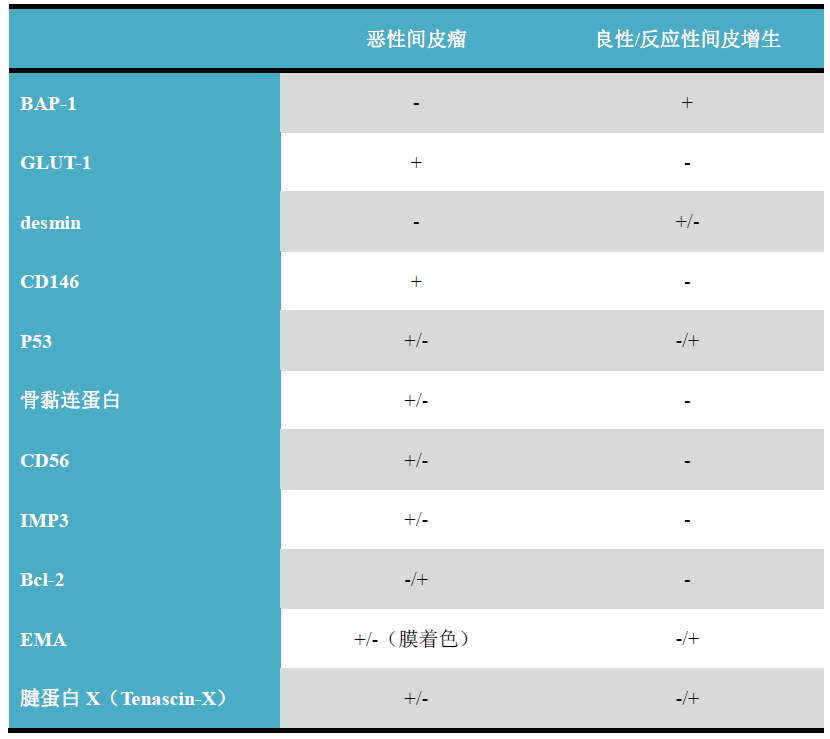
(Click to view larger image)
Detailed Explanation of Some Markers
All types of mesothelioma express broad-spectrum CK and CK5/6, CK7, CK8, CK10, CK14, CK18; but CK alone cannot distinguish mesothelioma from metastatic carcinoma. It is also important to note that submesothelial fibroblasts generally also express broad-spectrum CK and certain CKs, which may lead to misdiagnosis.
Positive expression pattern: Cytoplasm
Recommended positive control tissue: Appendix
Calretinin is a neuron-specific calcium-binding vitamin D-dependent protein expressed in various epithelial, mesenchymal, and central and peripheral nervous tissues. Because this marker is a neuron-specific related protein, it can be used to demonstrate ganglion cells in colon biopsy specimens for diagnosing Hirschsprung’s disease. This marker is strongly positive in normal and neoplastic mesothelial cells, making it an important mesothelial marker. It is also a marker for mast cells, steroid-producing cells, and tumors derived from these cells, such as granulosa cell tumor, Sertoli cell tumor, Leydig cell tumor, gonadoblastoma in sex cord-stromal tumors, and adrenal cortical tumors. About one-third of squamous cell carcinomas express calretinin to varying degrees. This marker is also widely expressed in various soft tissue tumors, such as synovial sarcoma, chondrosarcoma, desmoplastic small round cell tumor, lipoma, and liposarcoma. Because its expression spectrum is so broad, calretinin positivity alone is insufficient to diagnose mesothelioma.

Figure 1. Immunohistochemistry for calretinin clearly shows mesothelioma infiltrating the chest wall.
Positive expression pattern: Cell membrane
Recommended positive control tissue: Appendix
CD141, thrombomodulin (also known as endothelial anticoagulant protein), is a transmembrane glycoprotein expressed on the surface of endothelial cells, involved in regulating intravascular coagulation. This marker can be expressed in mesothelial cells, squamous epithelium, and transitional epithelium of the urinary tract, so it can be used for screening mesothelioma, transitional cell carcinoma, squamous cell carcinoma, and vascular tumors; but it is generally negative in sarcomatoid mesothelioma. Differential diagnosis of CD141-positive tumors is also crucial, and other specific markers should be added accordingly. CD141 is negative in renal cell carcinoma, prostate cancer, gastrointestinal adenocarcinoma, and endometrioid carcinoma.
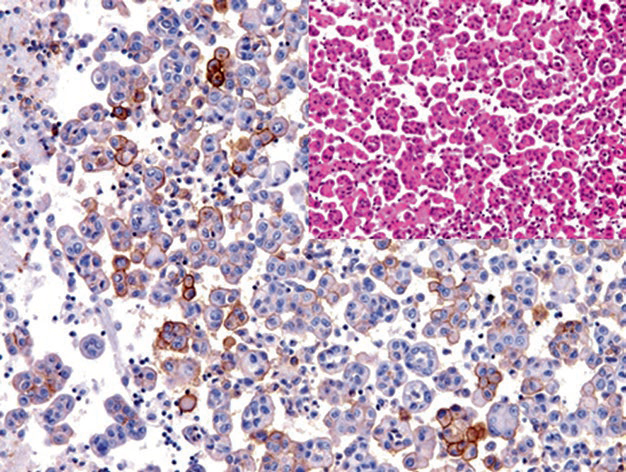
Figure 2. CD141 positivity in mesothelioma cells in malignant pleural effusion.
Positive expression pattern: Cell membrane
Recommended positive control tissue: Appendix
Mesothelin is a glycoprotein located on the surface of mesothelial and some other types of epithelial cells. Therefore, this marker is not only positive in mesothelioma but can also be expressed in other carcinomas, such as ovarian cancer, pancreatic cancer, lung cancer, and some adenocarcinomas. Generally, this marker is used for screening and should not be considered a specific marker for mesothelioma, and it is not expressed in sarcomatoid mesothelioma.
Regarding WT-1, it has been detailed in previous sections, and it is also an important mesothelial marker. WT-1 in mesothelioma shows nuclear positivity, so it can be used in double staining with other membrane-staining markers.
As mentioned, D2-40 (podoplanin) is a mucin expressed in lymphatic endothelial cells, but it is not specific; it can also be expressed in meningeal cells, germ cells, germ cell tumors, mesothelial cells, mesothelioma, and many other mesenchymal tumors.
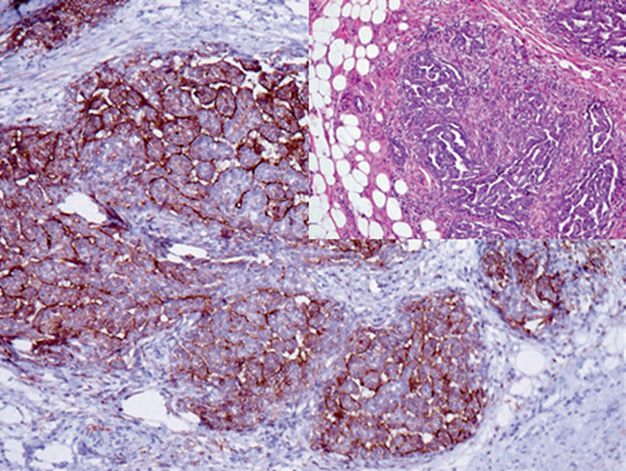
Figure 3. Immunohistochemistry for D2-40 clearly shows mesothelioma infiltrating the chest wall.
Positive expression pattern: Cell membrane
Recommended positive control tissue: Mesothelioma
This marker actually has no tissue specificity and is expressed in many epithelial and non-epithelial tumors. In practical diagnostic work, this marker may indicate malignant transformation, as it is overexpressed in many malignant epithelial and non-epithelial tumors. This marker also helps differentiate hemangioma (generally positive) from vascular malformations, pyogenic granuloma, and granulation tissue (which do not express GLUT-1). However, GLUT-1 is a hypoxia-inducible factor target gene, so its overexpression can also occur in hypoxic areas.
This marker is expressed in fetal tissues and various malignant precursor and malignant tissues; it is generally not expressed in benign adult tissues, except in the ovary, testis, placenta, endocrine cells, and brain tissue. In daily work, IMP3 is used to differentiate malignant from reactive hyperplastic lesions. Like GLUT-1, IMP3 also helps distinguish mesothelioma from reactive mesothelial hyperplasia, as most benign mesothelial cells do not express this marker.
IMP3 is also a marker for Hodgkin cells, but it can also be expressed in some parafollicular blasts or certain cells in B-cell lymphomas. Additionally, IMP3 helps differentiate endometrial serous carcinoma (positive) from endometrioid carcinoma (negative).

Figure 4. Malignant mesothelioma expresses IMP3.
BAP-1 is a transcriptional regulator and tumor suppressor. Deletions in different regions of the corresponding gene occur in various malignant tumors, such as mesothelioma, uveal and cutaneous malignant melanoma, renal clear cell carcinoma, lung adenocarcinoma, and meningioma. For different tumor types, loss of BAP-1 expression is associated with aggressive behavior. In routine immunohistochemistry, BAP-1 helps differentiate malignant mesothelioma and malignant melanoma (both lack nuclear BAP-1 positivity) from reactive mesothelial hyperplasia and benign melanocytic lesions (both are BAP-1 positive). When distinguishing benign from malignant lesions, literature reports its sensitivity as high as 90%; FISH detection of p16 also aids in this differentiation.
MaiMai Recommendation:”In this issue, we haveorganized and introduced the commonly used immunohistochemical markers for peritoneal tumor diagnosisA relatively systematic. In the specific diagnostic process, antibody selection is also very important, as the performance and quality of antibodies will affect the diagnostic outcome.”
|
Antibody Name
|
Clone Number
|
Positive Control
|
Cellular Localization
|
|
CK5&6*
|
MX040
|
Esophageal squamous cell carcinoma, Prostate
|
Cytoplasm
|
|
CK7*
|
MX053
|
Ovarian mucinous carcinoma, Lung adenocarcinoma
|
Cytoplasm
|
|
CK8*
|
MX004
|
Liver, Appendix |
Cytoplasm
|
|
CK14*
|
MX057
|
Lung squamous cell carcinoma, Esophageal squamous cell carcinoma
|
Cytoplasm
|
|
CK18*
|
MX035
|
Liver, Appendix |
Cytoplasm
|
|
Calretinin*
|
MX027
|
Mesothelioma, Appendix
|
Cytoplasm/Nucleus
|
|
D2-40
|
D2-40
|
Small intestine tissue, Mesothelioma |
Cytoplasm/Membrane
|
|
GLUT-1
|
SPM498
|
Placenta, Colon adenocarcinoma
|
Cell membrane
|
| IMP-3 |
EP286 |
Pancreatic cancer, Colon adenocarcinoma |
Membrane/Cytoplasm |
| WT-1* |
MX012 |
Kidney tissue, Wilms’ tumor |
Nucleus |
*Marked as Maixin clone product
For more information, please contact: 800-8581156 or 400-889-9853