
One Image to Understand: Consensus on Pathological Diagnosis of Gastrointestinal Adenomas and Benign Epithelial Polyps
Introduction:
With the widespread application of fiberoptic endoscopy technology, the detection rate of gastrointestinal polypoid lesions has significantly increased. Biopsy or resection specimens of gastrointestinal polypoid lesions have become one of the most common specimens in pathology departments. There are many types of gastrointestinal polypoid lesions. How can standardized and accurate pathological diagnosis of gastrointestinal polypoid lesions be achieved? At the beginning of 2020, the Digestive Diseases Group of the Chinese Society of Pathology released a consensus on the pathological diagnosis of gastrointestinal adenomas and benign epithelial polyps.
The editor has organized the diagnostic consensus related to gastrointestinal polypoid lesions into a diagram, hoping to provide clear and straightforward guidance for distinguishing related cases when encountered.

Click to enlarge the mind map for viewing
Schematic diagram of gastrointestinal lesion subtypes staining:

Figure 1 Gastric-type adenoma HE low magnification
Figure 2 Gastric foveolar-type adenoma HE low magnification
Figure 3 Gastric pyloric gland adenoma HE medium magnification
Figure 4 Gastric oxyntic gland adenoma HE medium magnification
Figure 5 Gastric fundic gland polyp, A and B: Endoscopic view showing solitary (A) or multiple (B), smooth-surfaced, broad-based gastric fundic gland polyps; C: Focal hyperplasia of oxyntic glands HE medium magnification
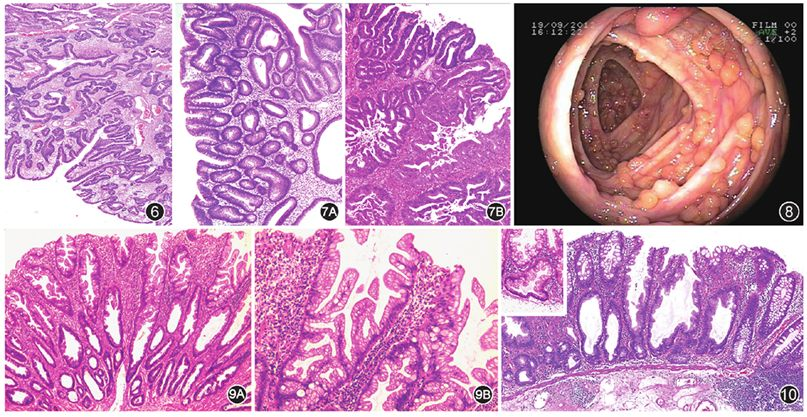
Figure 6 Hyperplastic polyp HE low magnification
Figure 7A Colorectal conventional adenoma HE low magnification
Figure 7B Colorectal conventional adenoma with high-grade dysplasia HE low magnification
Figure 8 Familial adenomatous polyposis, endoscopic view showing numerous adenomatous polyp lesions in the colon
Figure 9A Colorectal hyperplastic polyp HE low magnification
Figure 9B Colorectal hyperplastic polyp, serrated architecture at the luminal border HE medium magnification
Figure 10 Colorectal sessile serrated adenoma/polyp HE low magnification, top left corner HE high magnification
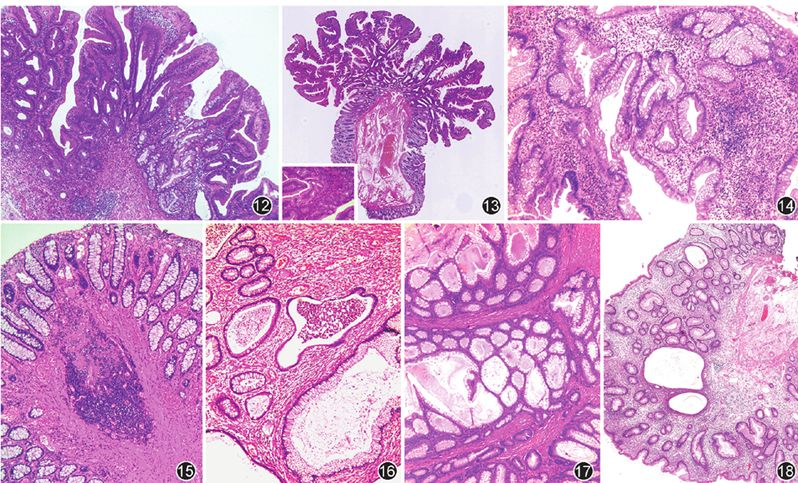
Figure 12 Sessile serrated adenoma/polyp (SSA/P) with serrated dysplasia, typical inverted T-shaped glands of SSA/P visible on the right HE low magnification
Figure 13 Colorectal traditional serrated adenoma, showing villous architecture, eosinophilic cytoplasm, and ectopic crypt formation HE low magnification, bottom left corner HE high magnification
Figure 14 Colorectal inflammatory pseudopolyp HE medium magnification
Figure 15 Colorectal mucosal prolapse-associated polyp HE medium magnification
Figure 16 Solitary juvenile polyp HE medium magnification
Figure 17 Peutz‑Jeghers polyp HE medium magnification
Figure 18 Cronkhite‑Canada syndrome polyp HE medium magnification