Steroidogenic factor 1 (SF-1/NR5A1/Ad4BP) is an orphan nuclear receptor and a member of the nuclear receptor superfamily. SF-1 is a major regulator of steroid metabolism, capable of activating the expression of all genes involved in cholesterol transport and steroidogenesis. SF-1 is normally expressed in tissues such as the hypothalamus, pituitary, adrenal glands, gonads, and skin. In pituitary adenomas, SF-1 is a gonadotroph lineage-specific transcription factor used to identify gonadotroph cell tumors.(GT)Gonadotroph cell adenomas are typically immunopositive for multiple hormones (FSH, LH), with about 20% of non-functioning gonadotroph adenomas identifiable only through SF-1 staining. Furthermore, SF-1 can distinguish silent gonadotroph adenomas (SGAs) from null cell adenomas (NCAs) and can reduce the incidence of NCAs to approximately 1%.
Silent gonadotroph adenomaand null cell adenoma differential diagnosis
The 2017 WHO new classification divides non-functioning pituitary adenomas (NFPAs) into silent pituitary adenomas (SPAs) and null cell adenomas (NCAs). Considering the potential clinical impact on patients, distinguishing NCAs from SGAs has clinical significance because NCAs are more invasive and have a poorer prognosis than SGAs. Balogun et al., in their cohort of 31 NCAs and 63 SGAs, detailed the differences in tumor behavior between these two subtypes, showing that NCAs are positively correlated with higher MIB-1 staining and pre- and postoperative tumor volume doubling times (TVDTs). In another retrospective study of 516 silent pituitary adenomas, 23.1% of SPA patients were initially classified as NCAs based on pituitary hormone immunohistochemistry. However, adding pituitary-specific transcription factors (SF-1, T-PIT, PIT-1) allowed reclassification of 95% of these patients into different lineages, reducing the prevalence of the NCA subtype to 1%.
SF-1 has prognostic significance
Surgical resection of gonadotroph tumors (GTs) is the most effective treatment, but some still recur. Hickman’s team reviewed the SF-1 immunohistochemical staining results of 51 GTs and reclassified them into 4 groups: Group 1—recently diagnosed GTs (n = 20), Group 2—non-recurrent GTs with long-term follow-up (n = 11), Group 3—initially resected recurrent GTs (n = 7), and Group 4—recurrent GTs (n = 13). They assessed the percentage of SF-1 immunolabeling in the lowest staining field (SF-1 labeling index, SLI) and performed RNA sequencing on GTs with SLI <80% and SLI >80%. Results: Diffuse strong positive staining for SF-1 was the most common pattern in Groups 1/2, while patchy SF-1 staining predominated in Groups 3/4. The median SLI in Groups 3/4 was lower than in Groups 1/2. Overall, GTs with SLI <80% recurred earlier than those with SLI >80%. They identified 89 statistically significant differentially expressed genes (FDR <0.05), including pituitary stem cell genes (SOX2, GFRA3) and various oncogenes (BCL2, ERRB4), which were overexpressed in GTs with patchy SF-1 expression. Conclusion: Patchy SF-1 staining reflects tumor heterogeneity in GTs and indicates relatively lower differentiation compared to GTs with diffuse staining. The SF-1 immunostaining pattern may have prognostic significance for GTs and could serve as an indicator for predicting recurrence.

Figure 1. Case 1 (Group 1): SF-1 and GATA3 show diffuse strong positive staining; Case 28 (Group 2): SF-1 shows diffuse strong positive staining, rare nuclear expression of GATA3 seen in F’; Case 34 (Group 3): SF-1 positive, perivascular distribution, negative for intranest mutation, GATA3 shows speckled staining; Case 35 (Group 3): scattered positive staining for SF-1 and GATA3 visible; M: SF-1 variable staining grades 1-4 within GT; N: Most recurrent tumors show patchy SF-1 staining, different from the non-recurrent group.
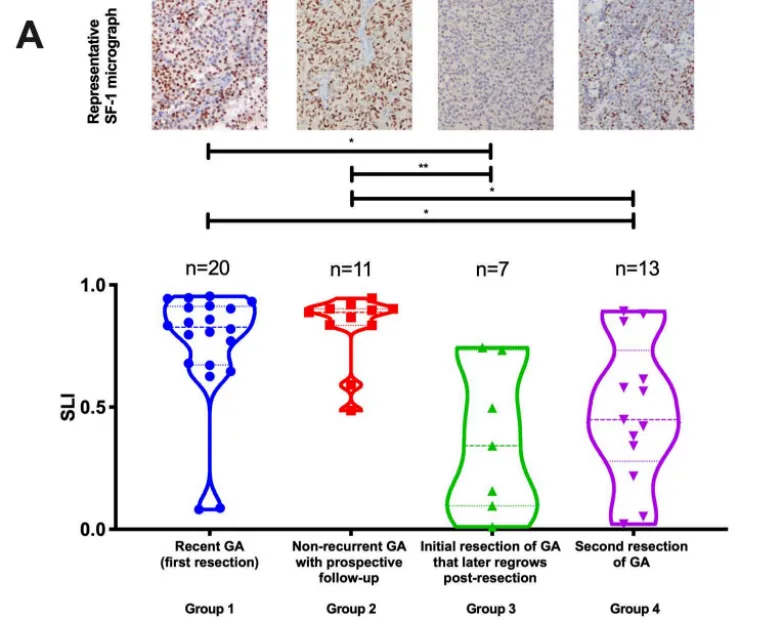
Figure 2. Analysis of SF-1 labeling index in different GT groups, dashed horizontal line reflects the median; Dunn’s test was used after Kruskal-Wallis test to determine significant difference levels, single asterisk (*) indicates p < 0.05, double asterisk (**) indicates p < 0.01; above are typical SF-1 staining images for each group.
Important clinical significance of SF-1
-
Precise diagnosis of gonadotroph tumor subtypes;
-
Differential diagnosis between silent gonadotroph adenoma and null cell adenoma;
-
Significance in guiding clinical prognosis judgment;
-
Reducing the cost of immunohistochemical testing for pituitary tumors;
According to the WHO new classification, based on morphology combined with immunohistochemical staining for specific hormones and transcription factors, the vast majority of pituitary adenomas can be classified without the need for ultrastructural analysis, as most ultrastructural features of tumors can be identified through immunohistochemistry, serving as a substitute to some extent. The SF-1 classic clone antibody (EP434) launched by Maixin, through multi-tumor multi-sample comparison, exhibits high specificity and high sensitivity for cell immunohistochemical detection based on gonadotroph differentiation, making it a valuable tool for aiding in the precise diagnosis of gonadotroph cell adenomas.
Maixin Related Antibodies
|
Antibody Name
|
Product Number
|
Clone Number
|
Cellular Localization
|
|
SF-1
|
RMA-1019
|
EP434
|
Nuclear
|
References:
【1】Iulia Florentina Burcea,Valeria-Nicoleta Năstase, Cătălina Poiană. (2021). Pituitary transcription factors in the immunohistochemical and molecular diagnosis of pituitary tumours — a systematic review. Endokrynologia Polska. Volume/Tom 72; Number/Numer 1/2021. DOI: 10.5603/EP.
【2】Hickman, R., Bruce, J., Otten, M., Khandji, A., Flowers, X., Siegelin, M., … Freda, P. (2020). Gonadotroph tumours with a low SF‐1 labelling index are more likely to recur and are associated with enrichment of the PI3K‐AKT pathway. Neuropathology and Applied Neurobiology. doi:10.1111/nan.12675
【3】Drummond, J., Roncaroli, F., Grossman, A. B., & Korbonits, M. (2018). Clinical and Pathological Aspects of Silent Pituitary Adenomas. The Journal of Clinical Endocrinology & Metabolism, 104(7), 2473–2489. doi:10.1210/jc.2018-00688

