
IKBCWG’s Recommendations for Ki-67 Assessment in Breast Cancer
Based on evidence presented in literature published over the past decade, IKBCWG recently proposed specific recommendations to address factors that may adversely affect the accuracy and reproducibility of Ki-67 assessment in breast cancer.The pre-analytical, analytical, and interpretative factors are summarized as follows (Table 3):
Table 3. Recommendations of the International Ki-67 in Breast Cancer Working Group
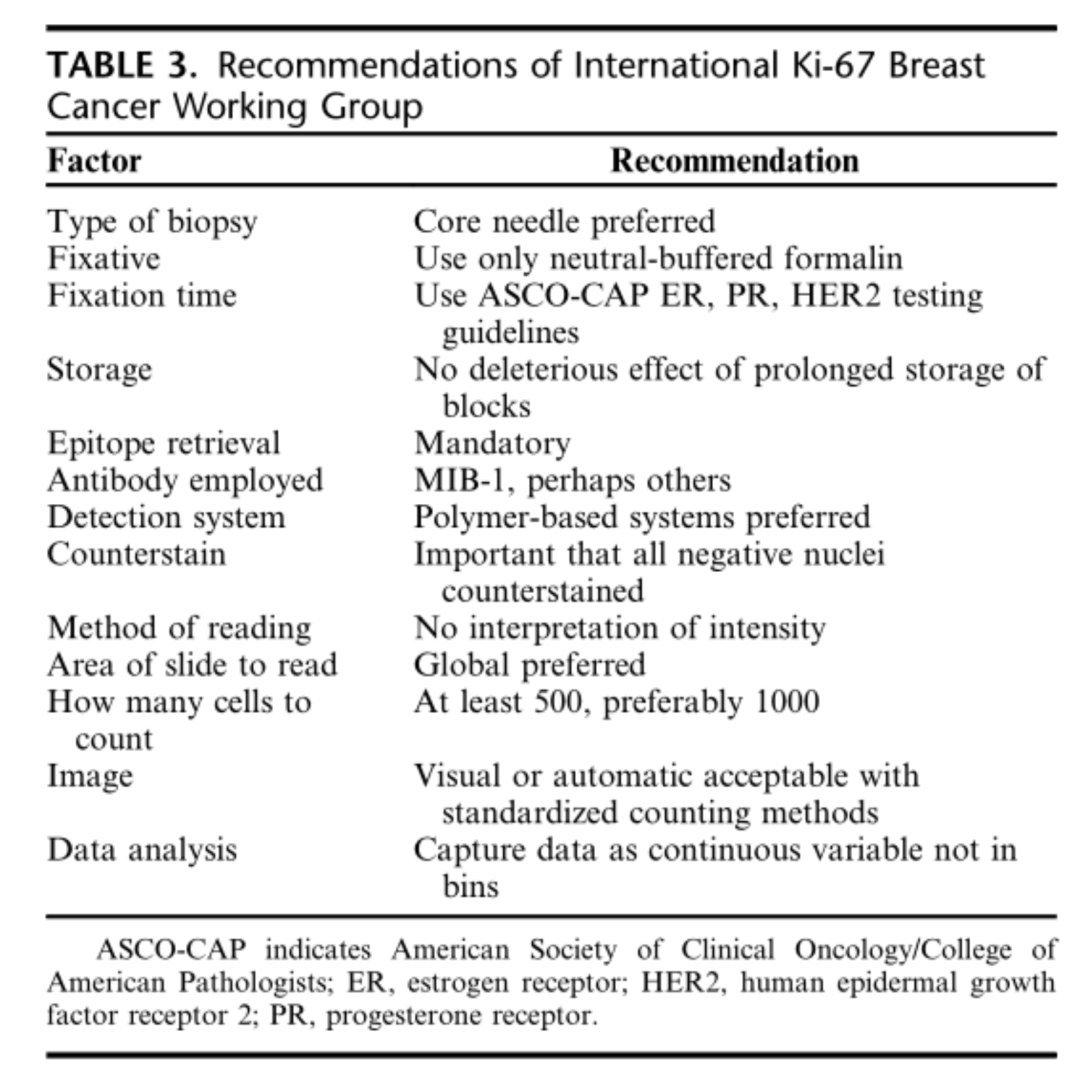
(1) Specimen Type: While both core needle biopsy and excision specimens may be suitable, recent evidence suggests core needle biopsy is preferred; this aligns well with recommendations for ER, PR, and HER-2 testing in breast cancer.
(2) Fixation: It has been documented that improper fixation and prolonged fixation time can lead to artificially low Ki-67 indices. It is recommended to follow the American Society of Clinical Oncology/College of American Pathologists (ASCO-CAP) guidelines for tissue processing for ER, PR, and HER-2, with fixation in neutral buffered formalin for at least 6 to 8 hours.
(3) Storage: Long-term storage of formalin-fixed, paraffin-embedded tissue at room temperature shows minimal adverse effects.
(4) IHC Antibody: MIB-1 is by far the most extensively validated antibody; anti-Ki-67 antibodies can be used if validated against MIB-1.
⑸IHC Method: It is recommended to use standard polymer-based detection systems rather than earlier avidin-biotin-based systems.
(6) Nuclear Counterstain: The counterstain (e.g., hematoxylin) should stain (making them countable) all Ki-67-negative nuclei.
(7) Scoring Method: Positive cell scoring should be independent of signal intensity.
(8) Number of Cells to Count: At least 500, preferably 1000 cells are recommended.
(9) Slide Reading Area: A global (average) score may be preferable to the hotspot method.
(10) Visual vs. Automated Cell Counting: Automated scoring shows high reproducibility with certain image analysis software, although visual scoring using standardized methods also shows high reproducibility. Both are acceptable at this time if performed properly.
(11) Dichotomization and Cutoff Values: Ki-67 index should be scored as a continuous percentage rather than in bins. For clinical decision-making, only consider ≥30% as high and ≤5% as low (see below).
Optimal Cutoff Values for “High” and “Low” Ki-67 Index
As mentioned, the assessment and inter-study comparison of Ki-67 index have proven to be major obstacles for Ki-67 index as a prognostic or predictive marker in breast cancer. Furthermore, the optimal cutoff value differs depending on the purpose of the assay (e.g., prognosis vs. prediction, response to neoadjuvant therapy vs. response to third-line therapy). The Gallen proposal to use a cutoff of 14% to separate luminal A from luminal B cancers and predict response to hormonal therapy remains controversial. While many researchers and clinicians adopt cutoffs between 10% and 20%, the IKBCWG recommendation is that if dichotomization of Ki-67 index is necessary for clinical decision-making, only tumors with an index of 5% or lower should be designated as “low” Ki-67 index, and those with an index of 30% or higher as “high” Ki-67 index.
Quality Assurance and Quality Control
It is strongly recommended that laboratories performing Ki-67 assessment on breast cancer specimens consider using recently described internal standards. Such laboratories should also participate in well-designed and implemented quality assurance and quality control programs. An excellent resource for those performing Ki-67 index assessment in the laboratory is the educational resource provided by IKBCWG at: https://www.ki67inbreastcancerwg.org/.
Abemaciclib is a CDK4/6 inhibitor recently approved by the U.S. Food and Drug Administration (FDA) for use in combination with endocrine therapy (ET) for the treatment of patients with ER-positive, HER-2-negative early breast cancer. Currently, this approval applies to patients with hormone receptor-positive, HER-2-negative, node-positive disease at high risk of recurrence and with a Ki-67 score ≥20% (measured by an FDA-approved test). The approval is based on data from the MonarchE trial, in which 5120 initial patients were randomized to ET with or without 2 years of Abemaciclib treatment. The use of this “FDA-validated” Ki-67 assay as a “companion diagnostic” for Abemaciclib has been controversial. Results from the MonarchE trial indicate that while the Ki-67 assay has prognostic significance, it does not actually predict a greater relative benefit from adding Abemaciclib.
Thus, the FDA’s first approval of a companion diagnostic for Ki-67 index determination has a prognostic role, but not a predictive one. Furthermore, the FDA approved this specific Ki-67 test with a designated cutoff of ≥20%, essentially determined visually without actual counting by manual or image analysis, which stands in stark contrast to the IKBCWG recommendations mentioned above.
Ki-67 is a powerful monoclonal antibody, defined as a cell proliferation marker for 40 years. While Ki-67 has been considered as a possible prognostic and predictive biomarker in the context of breast cancer, we still need a deeper understanding of it. Moreover, for Ki-67 index determination to become a reproducible and reliable biomarker, broader standardization and collaboration among pathologists, oncologists, pharmaceutical companies, and the FDA are required.
|
Antibody Name
|
Product Number
|
Clone Number
|
Cellular Localization
|
|
Ki-67
|
RMA-0731
|
MXR002
|
Nuclear
|
|
MAB-0672
|
MX006
|
Nuclear
|
References:
Gown Allen M.The Biomarker Ki-67: Promise, Potential, and Problems in Breast Cancer[J]. Applied Immunohistochemistry & Molecular Morphology, DOI:10.1097/PAI.0000000000001087.
For more information, please contact: 800-8581156 or 400-889-9853

