
Immunohistochemical Antibody Selection Scheme for Spleen Diseases (Part 2)
Introduction:
In the previous article, we provided a detailed introduction to the histology and flow cytometry of the spleen. This article will focus on the application of immunohistochemical antibodies in the differential diagnosis of common diseases involving the splenic white pulp, red pulp, and splenic interstitium, hoping to serve as a reference for colleagues in their daily work.
Common Diseases of Splenic White Pulp and Red Pulp
Splenic diseases are typically located in a specific area of the spleen, either the red pulp or white pulp. Splenic hamartoma, littoral cell angioma, hemangioma, and hairy cell leukemia (HCL) are commonly found in the red pulp, while other B-cell and T-cell lymphomas (such as splenic marginal zone lymphoma) are usually seen in the white pulp (Table 3). After identifying abnormalities in the red pulp and/or white pulp through routine HE staining and microscopic examination, a more specific immunohistochemical panel can be used for targeted differential diagnosis of lesions in that area. If there is red pulp abnormality, then CD8, CD68, CD163, CD31, CD34, ERG, WT1, DBA.44, annexin A1, T-bet, CD25, and BRAF can be used. If there is white pulp abnormality, using CD20, CD3, CD5, CD10, BCL6, BCL1, BCL2, and Ki-67 (also including MUM1, EBER, and CD30 when there is large cell infiltration) will be more helpful in distinguishing small B-cell lymphomas from large B-cell lymphomas (Table 1, see the first article).
|
Common Diseases of Red Pulp |
Common Diseases of White Pulp |
|
Splenic Hamartoma |
Splenic Marginal Zone Lymphoma |
|
Littoral Cell Angioma |
Diffuse LargeBCell Lymphoma |
|
Hemangioma |
Chronic Lymphocytic Leukemia/ Small Lymphocytic Lymphoma |
|
Hairy Cell Leukemia |
Measles |
|
Splenic Diffuse Red Pulp SmallBCell Lymphoma |
Typhoid Fever |
|
Chronic Myeloid Leukemia |
CastlemanDisease |
|
Infectious Mononucleosis |
Idiopathic Thrombocytopenic Purpura |
|
Angiosarcoma |
FeltySyndrome |
Splenic Interstitial Diseases
Although splenic interstitial lesions have a low incidence, they are the most common space-occupying lesions in the spleen and are often difficult to classify. The most common splenic interstitial lesion is splenic hemangioma, with an incidence of 0.02% to 0.16%. Hemangiomas are benign vascular tumors composed of interconnected endothelial cells with varying lumen sizes and shapes. By definition, hemangiomas lack malignant features such as solid areas, mitotic figures, cellular atypia, and necrosis, whereas splenic angiosarcomas possess these characteristics. There are two types of hemangiomas with intermediate malignant potential: hemangioendothelioma and Kaposi sarcoma. The appearance of splenic Kaposi sarcoma is similar to that of Kaposi sarcoma occurring in other sites, typically found in immunocompromised patients, most commonly HIV/AIDS (Acquired Immune Deficiency Syndrome). Kaposi sarcoma is positive for general vascular endothelial markers (i.e., ERG, WT1, CD31, CD34, and Factor VIII) but also positive for the lymphatic endothelial marker D2-40. Additionally, most cases are positive for human herpesvirus 8. Hemangioendothelioma can present in various forms, with tumor cells being epithelioid, spindle-shaped, or smooth muscle-like, and thus may be mistaken for epithelial or smooth muscle tumors. Splenic hemangioma, hemangioendothelioma, and angiosarcoma are all vascular tumors, so they can be stained with vascular markers (e.g., ERG, WT1, CD31, CD34, and Factor VIII). High-grade tumors, especially angiosarcomas, may lose some or most vascular markers; ERG is the most commonly retained marker in these tumors. Additionally, if it is an epithelioid hemangioendothelioma, keratin may be positive; if it is a smooth muscle-like hemangioendothelioma, SMA may be positive.
Due to similar histological morphology, lymphangioma often needs to be differentiated from hemangioma. Although lymphangiomas may contain some red blood cells, their lumens are often filled with pink proteinaceous fluid, whereas hemangioma lumens are typically filled with blood. Lymphangiomas are generally positive for vascular endothelial markers and also positive for D2-40, while hemangiomas do not express the latter.
Littoral cell angioma is a relatively rare vascular tumor found only in the spleen, believed to arise from red pulp sinus endothelial (littoral) cells. This tumor is located within the red pulp and consists of multiple irregular cystic lumens filled with blood. It may be multifocal and is most often discovered during abdominal imaging. The lumens are lined by tall columnar and flattened red pulp-derived cells that protrude into the vascular lumen. The tall columnar lining cells express histiocytic markers (CD68 and CD163), while the flattened cells express vascular markers (CD31 and Factor VIII). These tumors also express ERG but usually do not express WT1 and CD34. Compared to normal splenic littoral cells, littoral cell angioma does not express CD8. The co-expression of histiocytic and vascular markers is a distinctive feature of littoral cell angioma and can be used for differential diagnosis.
Splenic hamartoma is also unique to the spleen, with the lesion composed solely of red pulp, microscopically showing abundant red pulp without white pulp structures. On cut section, splenic hamartoma often protrudes from the surface to form a nodular mass pushing against adjacent normal spleen. Splenic hamartoma lacks a capsule but usually has a clear boundary with adjacent normal spleen. Structurally, it consists of various organized cords and sinus-like structures. The sinus lining cells are CD8 positive and also immunoreactive to general vascular endothelial markers (ERG, WT1, CD31, and Factor VIII). Additionally, they can show focal positivity for histiocytic markers (Figure 2, A to P).
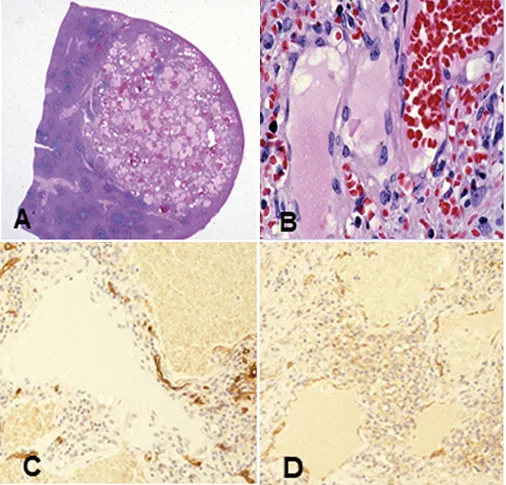
Figure 2 Vascular lesions involving the spleen. A to D, Hemangioma;
Figure 2A, Well-defined hemangioma;
Figure 2B, Abnormally dilated vessels with prominent endothelial cells;
Figure 2C, CD34 shows positivity in endothelial cells;
Figure 2D, CD31 shows positivity in endothelial cells.
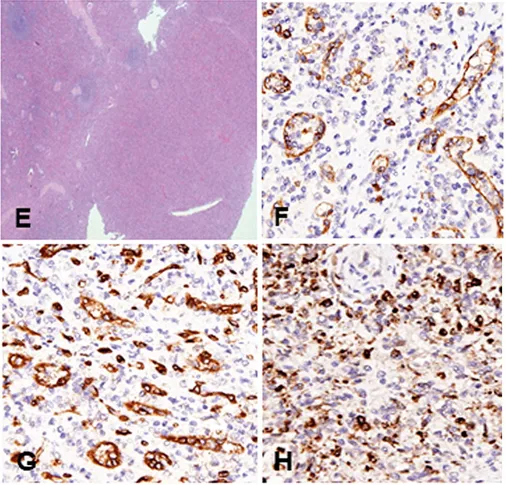
Figure 2E to H, Splenic hamartoma;
Figure 2E, Low-power view showing absence of white pulp structures;
Figure 2F, CD8 shows sinuses;
Figure 2G, CD34 shows normal splenic vessels;
Figure 2H, Lysozyme labels intrasinusoidal histiocytes.
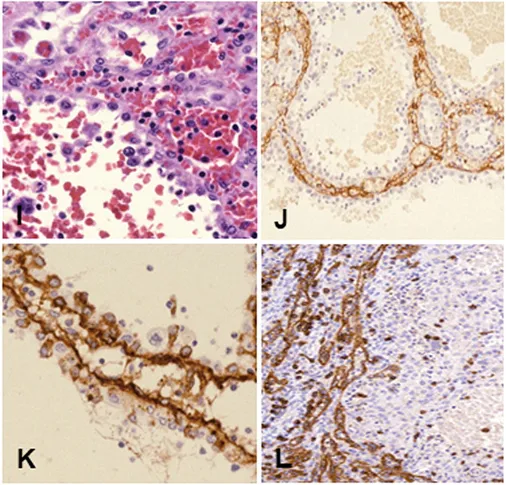
Figure 2I to L, Littoral cell angioma;
Figure 2I, Lining cells shedding into the vascular lumen;
Figure 2J, CD31 labels flattened endothelial cells;
Figure 2K, Factor VIII labels flattened cells;
Figure 2L, CD8 shows negativity in lining cells but stains splenic sinuses.
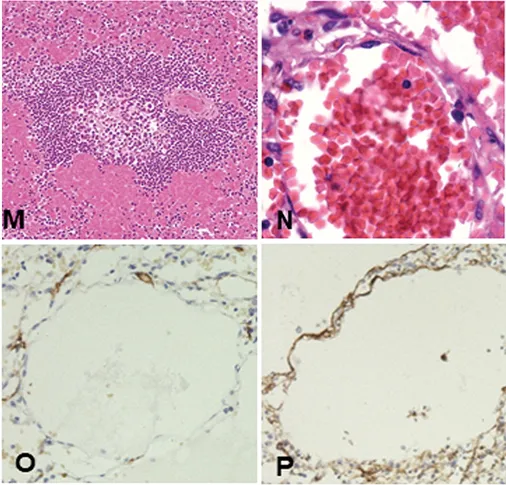
Figure 2M, Splenic sinus dilation, adjacent to a white pulp nodule.
Figure 2N, Red blood cell filling causes splenic sinus dilation.
Figure 2O, CD34 shows negativity in lining cells.
Figure 2P, Factor VIII shows staining of splenic sinuses.
To be continued.…..
Related Antibodies from Maixin
|
Antibody Name |
Product Number |
Clone Number |
Positive Location |
|
CD5* |
MAB-0827 |
MX052 |
Cell Membrane |
|
CD5 |
Kit-0033 |
SP19 |
Cell Membrane |
|
CD10* |
MAB-0668 |
MX002 |
Cytoplasm/Cell Membrane |
| CD30 |
MAB-0023 |
Ber-H2 |
Cytoplasm/Cell Membrane |
|
CD31* |
MAB-0720 | MX032 | Cell Membrane |
| CD68 | Kit-0026 | KP1 |
Cytoplasm |
| CD163 | MAB-0206 |
10D6 | Cell Membrane |
*Indicates Maixin clone product