
Normal breast tissue includes stromal components and epithelial components, and the epithelial components can be further divided into three different cell types: ducts, acini, and myoepithelial cells. The immunophenotypes of different components have their own characteristics, so tumors derived from different components also have different immunophenotypes, which is an important theoretical basis for immunohistochemical testing of breast tumors.
In addition, breast neoplastic lesions have diverse morphologies, so in practical work, relevant indicators should be selected purposefully according to different objectives. Details are shown in Tables 1-3.
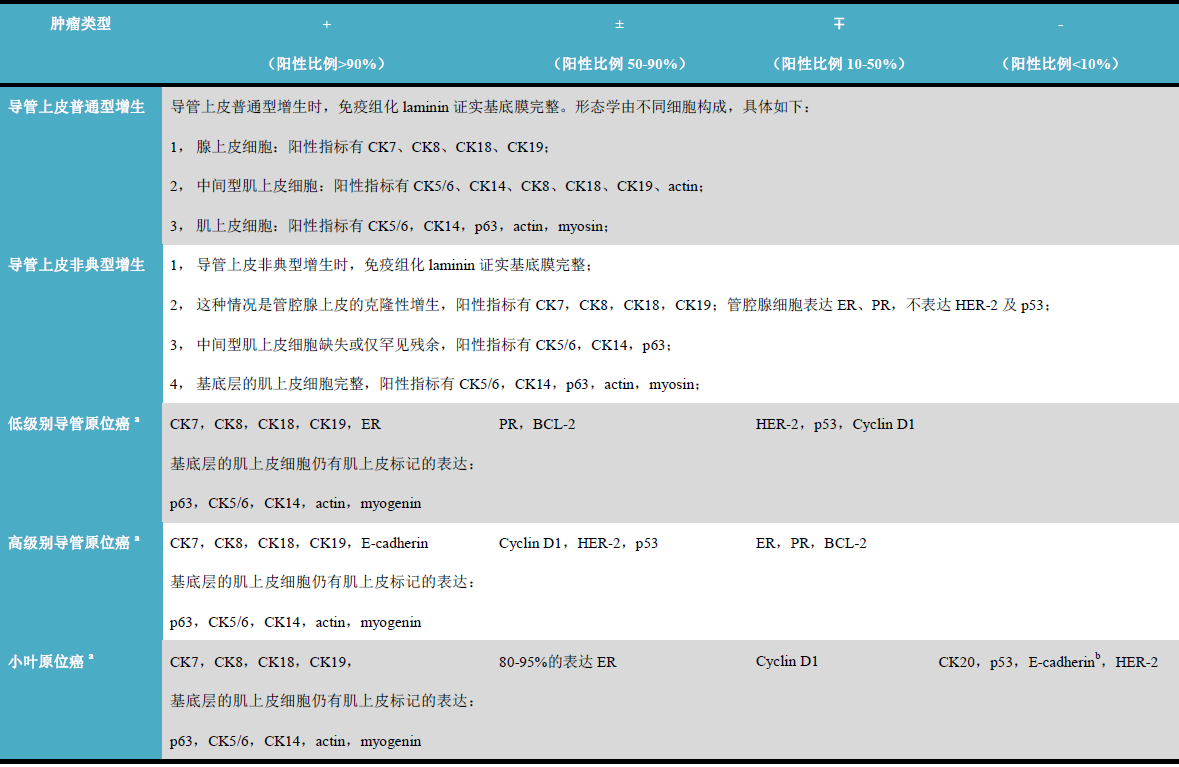
Table 1. Immunohistochemical characteristics of breast ductal epithelial hyperplasia and carcinoma in situ
(Click to view larger image)
Note:
-
Intermediate myoepithelial cells are absent or only a few remnants on the luminal surface, with positive immunohistochemical indicators being CK5/6 and CK14; the basal myoepithelial layer is intact, with positive immunohistochemical indicators being CK5/6, CK14, p63, Actin, myogenin, h-caldesmon, and calponin.
-
Normal non-neoplastic breast lobular cells are E-cadherin positive.
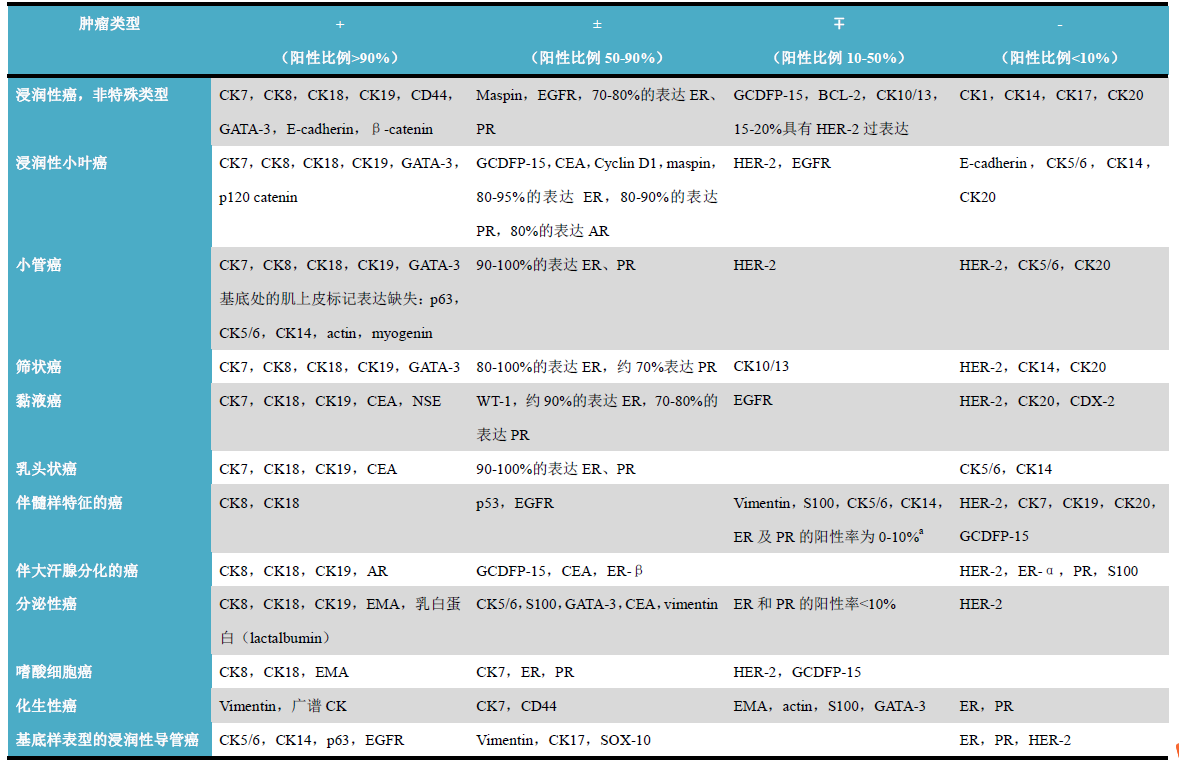
Table 2. Immunohistochemical characteristics of breast invasive carcinoma
(Click to view larger image)
Note:
-
In typical medullary carcinoma, ER and PR are generally negative.
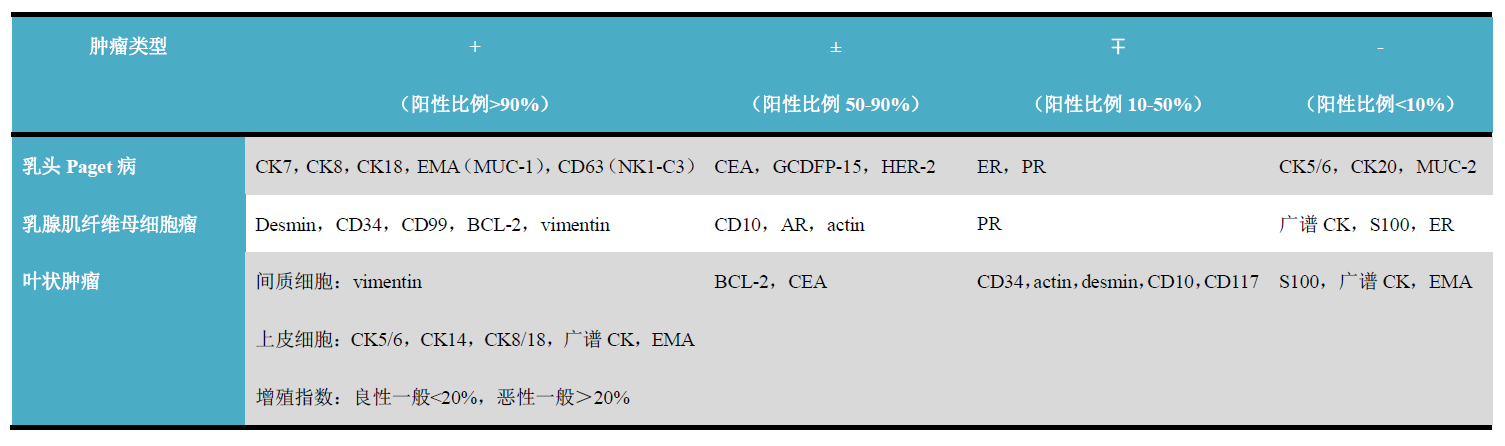
Table 3. Immunohistochemical characteristics of other breast tumors
(Click to view larger image)
Detailed explanation of some indicators
Positive expression pattern: Nucleus
Recommended positive control tissue: Normal breast tissue
ER is a member of the steroid hormone receptor family, specifically including two types encoded by different genes: ER-α and ER-β. The distribution of different types of ER varies in different organs and tissues of the human body: ER-α is mainly expressed in epithelial and stromal cells of the breast, uterus, placenta, liver, central nervous system, vascular endothelium, bone tissue, etc., while ER-β is mainly expressed in the prostate, testis, ovary, spleen, thymus, skin, and endocrine glands (such as thyroid, parathyroid, adrenal, pancreas). Of course, many tissues also express both types of ER.
Based on the aforementioned information, ER expression can serve as a good immunohistochemical marker for most breast cancers and certain cancers of uterine and ovarian origin. For all steroid receptor markers, staining patterns other than nuclear staining should be interpreted as negative.
The expression of ER-α in breast cancer also has predictive significance for endocrine therapy efficacy; whether ER-α is expressed also provides some guidance for the selection of other treatment options and patient prognosis. Currently, there are several semi-quantitative scoring schemes for ER and PR, and their scoring systems are basically calculated based on nuclear staining intensity and the proportion of positive tumor cells. In the 2019 fifth edition of the World Health Organization classification of breast tumors, the assessment principle for ER-α is: as long as 1% of tumor cells are weakly positive, it can be assessed as positive, because evidence suggests that this group of cases may also benefit from endocrine therapy. However, invasive carcinomas with a tumor cell positivity proportion of 1-10% should be reported as low positive with further notes. At the same time, given the heterogeneity of ER expression in breast cancer, attention should be paid to reporting the proportion of positive cells among all invasive carcinoma components; if there are differences in positivity levels, a comprehensive assessment of the overall positive staining should also be noted.
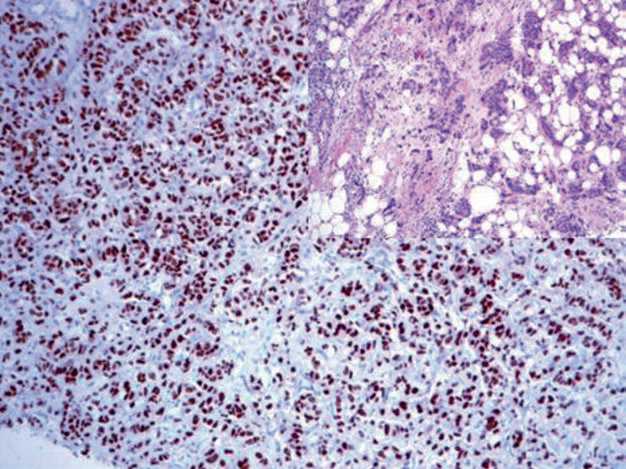
Figure 1. Breast cancer, strong positive nuclear expression of ER.
The expression of ER in breast cancer is related to tumor histological type and differentiation degree. In addition, ER expression is not limited to the above-mentioned organs and tissue types and may also be expressed in other tumors, such as hepatocellular carcinoma and transitional cell carcinoma. Therefore, in practical applications for diagnosing primary breast cancer, attention should be paid to adding more markers, such as GATA-3, Mammaglobin, GCDFP-15, PR, and some CKs.
Positive expression pattern: Nucleus
Recommended positive control tissue: Normal breast tissue
Progesterone is a steroid hormone related to the differentiation of breast parenchyma and endometrium. PR is a good marker for breast cancer. Since this marker is expressed in only a few non-breast cancer tumor types, its sensitivity for breast cancer diagnosis is better than that of ER. Similar to ER, PR expression is related to tumor differentiation degree; high-grade cancers mostly have negative hormone receptors. At the same time, PR status is also an important prognostic indicator for breast cancer, endometrial cancer, and ovarian cancer. High-level expression of ER and PR indicates better endocrine therapy efficacy for breast cancer and endometrial cancer.
Positive expression pattern: Cell membrane
Recommended positive control tissue: HER-2 positive tumor/brain tissue
The HER-2 molecule is part of the cell membrane of normal epithelial cells, with a small number of receptors. In cancer, amplification of the HER-2 gene located on chromosome 17 leads to overexpression of the corresponding marker on the tumor cell membrane. However, this characteristic is only seen in a few tumor types, mainly breast cancer, gastric adenocarcinoma, and a few other cancers, such as ovarian cancer, non-small cell lung cancer of the lung, adenocarcinoma, and transitional cell carcinoma of the urinary tract.
HER-2 gene amplification can be detected by FISH. Since immunohistochemistry can simply assess the overexpression of HER-2 molecules on the tumor cell membrane, semi-quantitative detection can also be achieved through specific antibodies. HER-2 immunohistochemistry results have become an important indicator in the treatment of breast cancer and other HER-2 positive cancers. To accurately assess HER-2 expression, the following issues should be noted:
-
Tissues used for HER-2 immunohistochemistry must be extremely well fixed;
-
Assessment of immunohistochemistry results must be performed with reference to standard control slides scored as 0, 1+, 3+;
-
Only membrane staining is recorded as positive; cytoplasmic or nuclear staining must be ignored, and edge artifact staining in immunohistochemistry should also be ignored;
-
Only the invasive component of the tumor should be assessed.
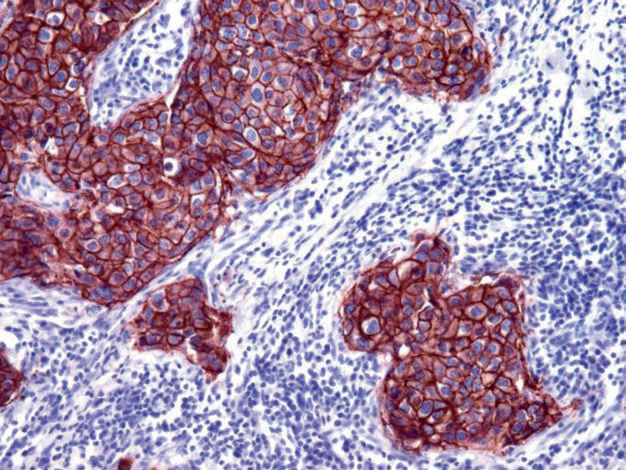
Figure 2. Breast cancer, all tumor cells in this image show strong positive HER-2 expression, scored as 3+.
For specific scoring, interpretation of related results, and further management of HER-2 in breast cancer, please refer to the latest relevant guidelines. It should be noted that HER-2 is not a specific marker for breast tissue and breast cancer, and only about 30% of breast cancers show HER-2 overexpression, mainly high-grade cancers of non-special type.
Positive expression pattern: Nucleus
Recommended positive control tissue: Normal breast tissue
GATA-3 is involved in the regulation of breast luminal epithelial proliferation and differentiation, as well as in the differentiation of T lymphocytes and skin appendages. In clinical practice, GATA-3 is widely used in the diagnosis and differential diagnosis of primary and metastatic breast cancer and transitional cell carcinoma. Up to 90% of breast cancers express GATA-3, but the positivity rate is lowest in triple-negative breast cancer, and also low in metaplastic breast cancer and sarcomatoid breast cancer. In male breast cancer, the GATA-3 positivity rate is only one-third. Strong positive expression of GATA-3 in breast cancer is also accompanied by ER expression; high expression of GATA-3 generally indicates a better prognosis.
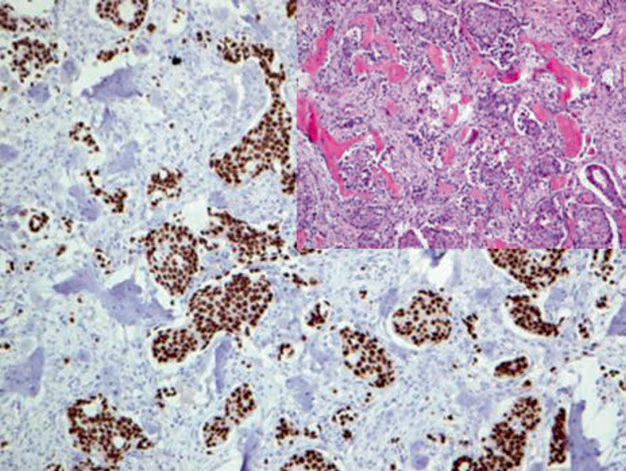
Figure 3. Breast invasive ductal carcinoma, bone metastasis; immunohistochemistry shows strong positive nuclear expression of GATA-3 in tumor cells.
As mentioned earlier, GATA-3 can also be applied to the diagnosis and differential diagnosis of primary and metastatic transitional cell carcinoma, which will be detailed later in this series of articles. However, besides these, many other tissues and tumors express GATA-3, and caution should be exercised in interpretation to avoid pitfalls. Specifically, mesothelioma, squamous cell carcinomas of various organs, pancreatic ductal adenocarcinoma, skin appendage tumors, and various benign and malignant salivary gland tumors (such as salivary duct carcinoma, acinic cell carcinoma, adenoid cystic carcinoma, epithelial-myoepithelial carcinoma) show varying degrees of GATA-3 expression. It has also been reported that a few endometrial cancers express GATA-3. GATA-3 expression is also characteristic of T lymphocytes and peripheral T-cell lymphoma. Notably, reactive mesothelium also expresses GATA-3. Due to these issues, the specificity of GATA-3 should be considered when used for breast tumor and urothelial tumor diagnosis.
Positive expression pattern: Cytoplasm
Recommended positive control tissue: Normal breast tissue
Mammaglobin is a low molecular weight protein, and monoclonal antibodies against this protein are good markers for breast-derived tumors: 80-90% of primary breast cancers and lymph node metastases express this marker.
Like other breast markers, Mammaglobin expression is not limited to breast tissue and corresponding tumors but can also be seen in other tumor types, such as endometrioid carcinoma, sweat gland carcinoma, salivary gland tumors, a few cholangiocarcinomas, and lung adenocarcinoma. Mesothelioma does not express Mammaglobin.
Positive expression pattern: Cytoplasm
Recommended positive control tissue: Breast tissue/skin (apocrine cells)
This protein is expressed in apocrine cells or cells with apocrine metaplasia and is regulated by the androgen receptor. Therefore, this antibody can be expressed in apocrine cells and related tumors in multiple sites. Breast ductal and lobular cells do not express GCDFP-15. The positivity rate of GCDFP-15 in breast cancer varies in different studies, generally ranging from 30% to 90%. Triple-negative breast cancer generally does not express GCDFP-15.
GCDFP-15 can also be expressed in other apocrine, eccrine, and serous glandular epithelium and cancers derived from these glands, such as skin appendage tumors; this should be considered when differentiating primary skin tumors from metastatic breast cancer.
E-cadherin is a transmembrane glycoprotein and a major member of calcium-dependent cell adhesion molecules. E-cadherin expression is related to epithelial stratification, polarization, and gland formation. E-cadherin is expressed in many types of epithelial cells and related cancers. In routine histopathology, E-cadherin is used to differentiate breast ductal carcinoma and lobular carcinoma: breast lobular tumors do not express E-cadherin. The loss of E-cadherin expression in breast lobular tumors leads to the accumulation of cytoplasmic p120 catenin, which can also serve as a marker for breast lobular carcinoma. E-cadherin can also be used to differentiate reactive mesothelial hyperplasia from mesothelioma, with the former generally negative and the latter generally positive. E-cadherin can also serve as a prognostic indicator for various types of cancers, such as breast cancer and transitional cell carcinoma, because the loss of E-cadherin expression is associated with aggressive behavior.
This indicator is a breast differentiation antigen, expressed in normal breast epithelium and60%breast cancer. Immunohistochemical expression pattern is cytoplasmic staining, occasionally nuclear staining; its staining intensity is related to tumor differentiation degree andERexpression level. Apocrine glands and about one-third of apocrine tumors can also expressNY-BR-1。
Mai Mai:”E-Cadherin is almost always positively expressed in all ductal carcinoma in situ and invasive carcinomas, while it is often negative in lobular carcinoma in situ and invasive carcinomas. Combined use with p120 can be used for differential diagnosis between breast ductal carcinoma and lobular carcinoma. AndMost patients with ER and PR positive tumors respond well to endocrine therapy, with high remission rates, low recurrence rates, and good prognosis.ER is oftenused together withPR and HER-2 as routine examination items for breast cancer patients. Mammaglobin has high specificity in breast tissue and is positively expressed in 80% of breast cancers. Combined use with GCDFP-15 can be used for breast cancer diagnosis.”
|
Antibody Name
|
Clone Number
|
Positive Control
|
Positive Location
|
|
E-Cadherin*
|
MX020
|
Breast invasive ductal carcinoma, liver
|
Membrane/cytoplasm
|
|
ER
|
SP1
|
Breast cancer, cervix
|
Nucleus
|
|
GATA-3
|
L50-823
|
Urothelial carcinoma, breast cancer
|
Nucleus
|
|
GCDFP-15
|
23A3
|
Salivary gland tissue, breast tissue
|
Cytoplasm
|
|
HER-2*
|
MXR001
|
Breast invasive ductal carcinoma
|
Membrane
|
|
Mammaglobin
|
304-1A5
|
Breast tissue
|
Cytoplasm
|
|
PR
|
SP2
|
Breast cancer, endometrium
|
Nucleus
|
*Marked as Maixin clone product
For more information, please contact: 800-8581156 or 400-889-9853
