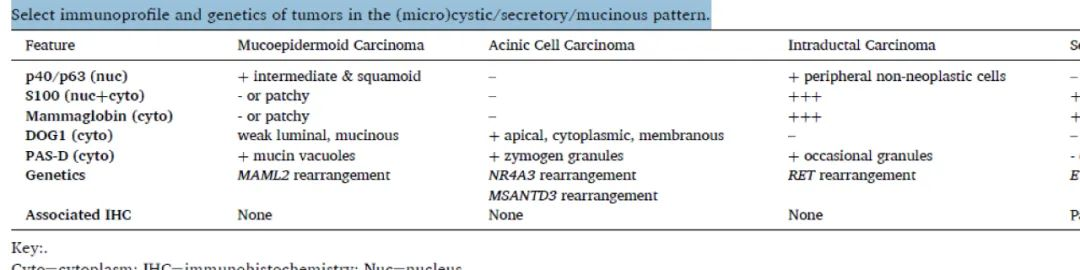
(micro)cystic/secretory/mucinous
These tumors [Table 1] typically exhibit uniform cytomorphology, with structures ranging from microcystic to cystic, sometimes solid. The cystic spaces may contain intraluminal secretions, and cells may show intracytoplasmic vacuoles or granular material. These lesions include mucoepidermoid carcinoma (MEC), acinic cell carcinoma (AcCC), secretory carcinoma (SEC), and intraductal carcinoma (IDC). MEC is the only salivary gland tumor with three cell types: mucinous cells, intermediate cells, and squamous cells. However, the distinction between the latter two may be unclear. The architecture can range from microcystic, to macrocystic, to solid. Although AcCC is usually solid, true microcystic variants can pose diagnostic challenges,but intracytoplasmic zymogen granules should be present.Microcystic, papillary, solid growth patterns are seen, with watery or dense secretory material in the lumina, occasionally with intracytoplasmic non-mucinous vacuoles.IDC often has numerous large cystic structures with intraluminal proliferative growth, uniformly surrounded by an outer myoepithelial/basal cell layer.Polymorphous (cribriform) adenocarcinoma (discussed in the basaloid/tubular/cribriform section) can show microcystic areas and should also be considered in the differential diagnosis.
Table 1. Immunophenotype and genetics of (micro)cystic/secretory/mucinous tumors
(Click to view larger image)
Evaluation of myoepithelial/basal markers (p40/p63) may again provide a starting point. MEC diffusely expresses p40/p63 in most cells (including intermediate and squamous cells) (Figure 1). The unique feature of IDCis that all nests are surrounded by a single layer positive for p40/p63/SMA/calponin, confirming the intraductal location.The lesional cells proliferate within the confines of the ductal system; however, occasional cases with focal invasion have been reported.AcCC and SEC are negative for p40/p63 as they both consist of a single cell type.
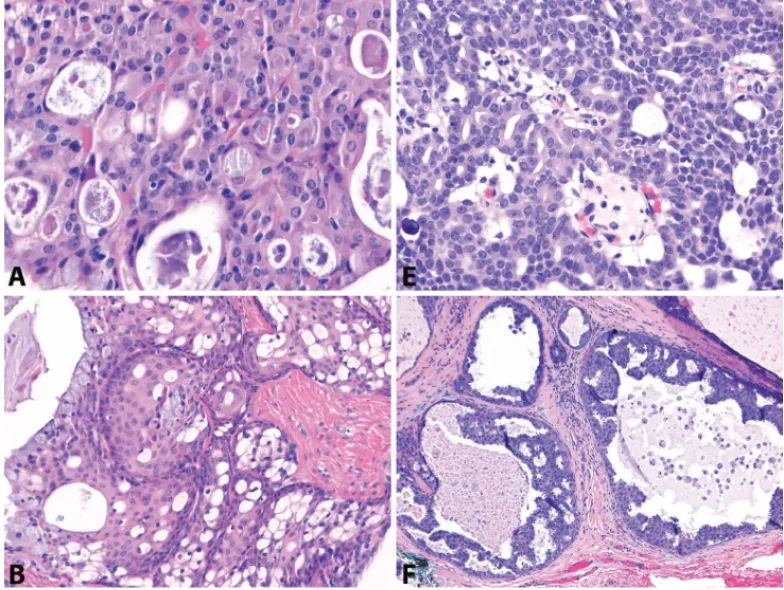
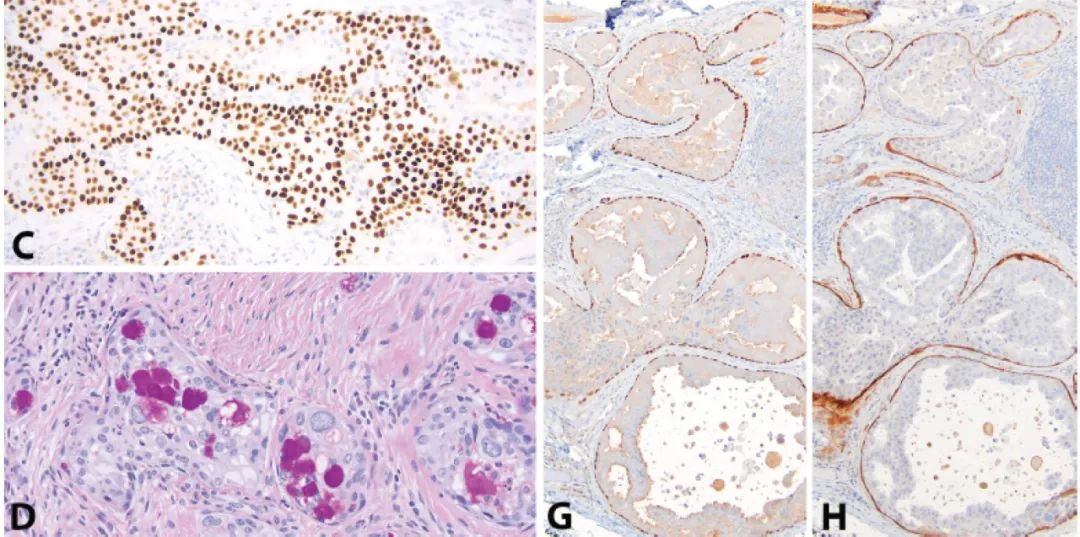
Figure 1: Mucoepidermoid carcinoma vs. Intraductal carcinoma. At high power, some mucoepidermoid carcinomas (A) and intraductal carcinomas (E) can show microcystic architecture. However, low power reveals more characteristic macrocystic and solid areas in mucoepidermoid carcinoma (B), and intraductal proliferation and intraluminal growth in intraductal carcinoma (F). Most mucoepidermoid carcinoma cells express p63 (C), while only the non-neoplastic peripheral cell layer is positive in intraductal carcinoma (G). These peripheral myoepithelial cells also express SMA (H). PAS-positive, diastase-resistant intracytoplasmic mucin vacuoles are present in mucoepidermoid carcinoma (D), but caution should always be exercised as mucinous metaplasia can occur in many other salivary gland tumors.
S100 and mammaglobin are particularly useful in this category, as both SEC and IDC exhibit strong and diffuse expression. [Figure 2] AcCC is negative. MEC may show patchy non-specific staining.Androgen receptor may also be expressed in the apocrine secretory variant of IDC.DOG1 immunostaining and PAS/PAS-diastase histochemical stains are also helpful for this pattern group.DOG1 is typically expressed in AcCC, showing apical membranous, cytoplasmic, or complete membranous staining.Patchy staining can be seen in luminal and mucinous cells of MEC and other non-AcCC tumors (PA, PAC, AdCC).DOG1 is negative in IDC and SEC.Intracytoplasmic mucin in MEC and zymogen granules in AcCC are both PAS-positive/diastase-resistant.
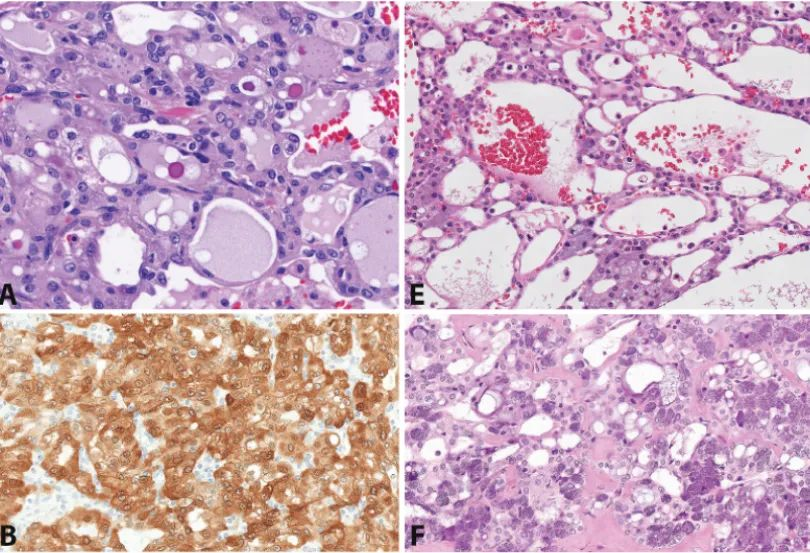
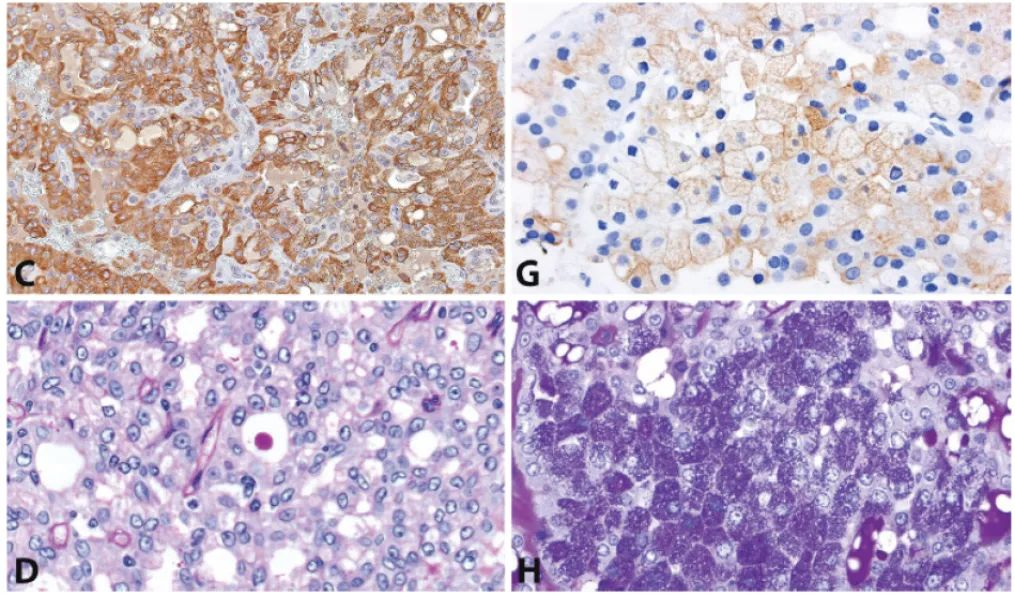
Figure 2: Secretory carcinoma vs. Acinic cell carcinoma. Secretory carcinoma (A) in most cases shows diffuse strong S100 (B) and mammaglobin expression (C). In contrast, acinic cell carcinoma, including true microcystic variants (E), is negative for both. The presence of serous acinar cells, even focally, aids in diagnosis (F). In acinic cell carcinoma (G), DOG1 shows variable apical membranous or cytoplasmic expression, while it is negative in secretory carcinoma. PAS-positive, diastase-resistant intracytoplasmic granules are absent in secretory carcinoma (D), even though intraluminal secretions may be highlighted. Diastase-resistant zymogen granules are present in acinic cell carcinoma (H).
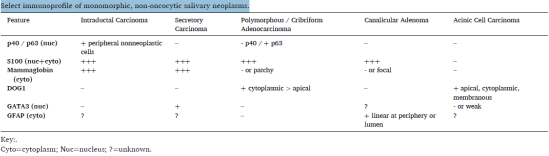
While PAS-D can stain intraluminal secretions in SEC, it should not highlight cytoplasmic contents. In some IDC, PAS-D shows intracytoplasmic granules. A reported pitfall includes the presence of PAS-D-positive pseudo-zymogen or hemosiderin granules in SEC, which can be confirmed by iron stain. The discussion of strong and diffuse S100 expression is incomplete without re-mentioning PAC and introducing tubular adenoma. Tubular adenoma predominantly occurs on the upper lip of middle-aged to elderly women. It consists of slender cords of cuboidal to columnar cells, occasional beading, cyst formation, and loose myxoid vascular stroma. S100 and GFAP show diffuse expression around the tumor or cystic spaces. Table 2 provides an overview of monomorphic tumors (including those expressing S100).
Table 2. Immunophenotype of monomorphic, non-oncocytic salivary gland tumors
(Click to view larger image)
Genetic analysis may aid this morphological group; however, immunohistochemical correlates are scarce. MEC typically harbors MAML2 gene rearrangements, most commonly with fusion partners CRTC1 and CRTC3. There is no immunohistochemical correlate for MAML2. IDC often shows RET rearrangements, with the most common fusion partners being NCOA4 in the conventional intercalated duct phenotype and TRIM27 in the apocrine secretory phenotype. Similarly, RET rearrangements lack immunohistochemical correlates. Recently, NR4A3 or less commonly MSANTD3 gene rearrangements have been identified in AcCC. Cases with NR4A3 rearrangement may show nuclear expression with NR4A3 immunostaining, while NR4A3 immunostaining is negative in other evaluated salivary carcinomas. There is no immunohistochemical correlate for MSANTD3. ETV6-NTRK3 rearrangement is present in most SEC, along with ETV6 rearrangements with RET and other unknown partners. Other anatomical sites (breast, skin, thyroid, lung) are histologically and genetically identical. Cases with ETV6-NTRK3 rearrangement should show nuclear expression with pan-TRK immunostaining. Cytoplasmic or membranous expression has been documented in MEC, PA, and PAC. Molecular confirmation of TRK gene rearrangements may indicate prior to treatment with TRK inhibitors.

