
Carcinoma of unknown primary (CUP) is a malignancy diagnosed as metastatic butPrimary sitewith an unknown primary site. CUP prevalence accounts for about 4% of all cancers, often presenting as metastases to lymph nodes, lung, liver,Metastases to the liver, bone, brain, solid organs, and peritoneal or pleural cavities.
In the IHC diagnosis of CUP, although the CK7 and CK20 combination is commonly used as the first step in cancer evaluation, with four expression patterns(CK7+/CK20+,CK7+/CK20-,CK7-/CK20+,CK7-/CK20-), butTo performa definitive diagnosis should also be supported by organ-specific markers.
This retrospective investigation aimed to evaluate thethe frequency and accuracy of each IHC marker for CUP.
A retrospective analysis and IHC study were conducted on all CUP patients with complete data at Shahid Faghihi Hospital from 2015 to 2020 (malignant melanoma, sarcoma, germ cell tumors, neuroendocrine carcinoma, and mesothelioma were excluded from the study).。
Among the 595 collected CUP cases, 307 were eligible for this study. The most common site of presentation for CUP was the liver, but the primary source could not be determined in 27% of cases. The frequency of primary organs in metastatic cases is shown in Figure 1.
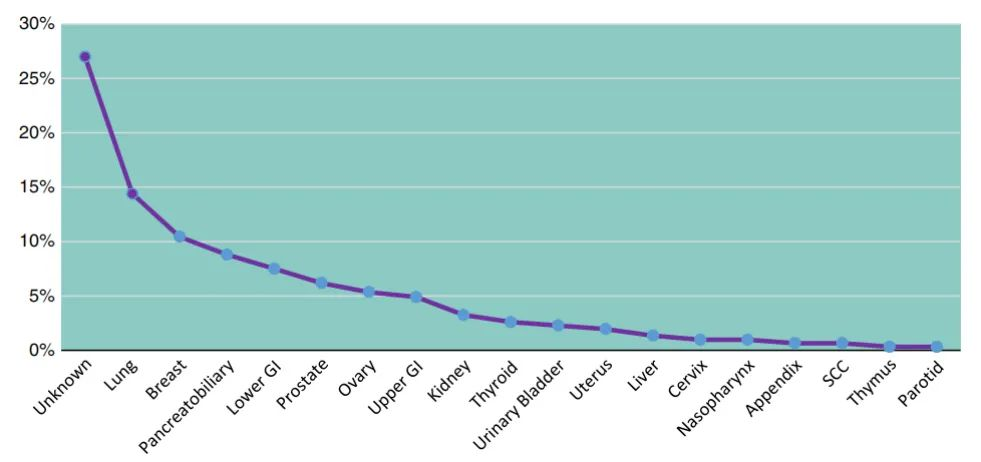
Figure 1. Frequency of primary organs in metastatic carcinoma
The results showed,99.4% of CUP cases were CK positive,with only one case being CK negative. CK7/CK20 expression was tested in 262 cases, and their different expression patterns were evaluated, as shown in Figure 2.
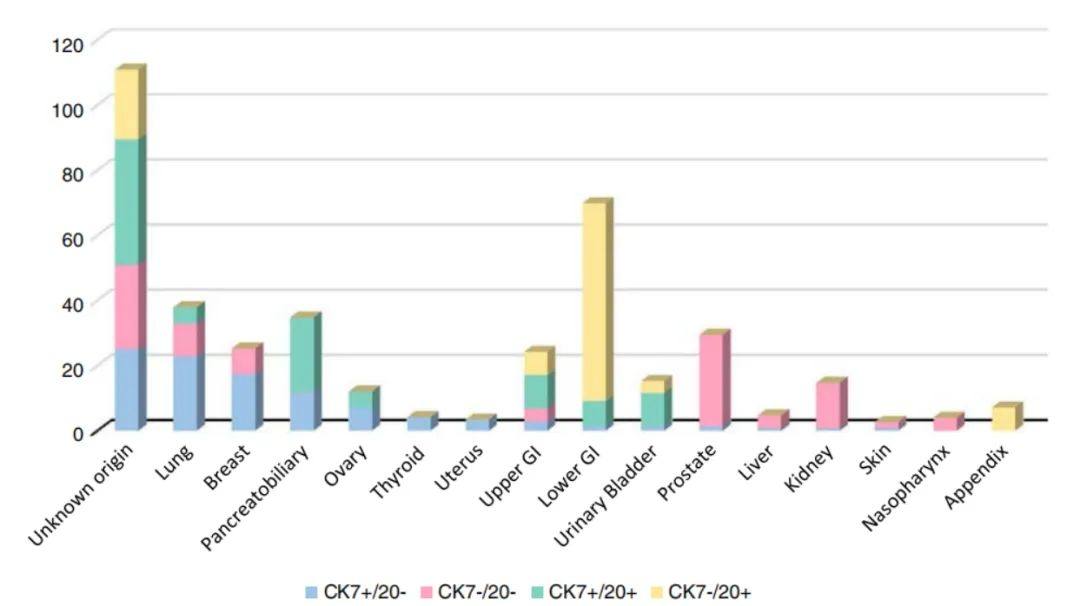
Figure 2. Different expression patterns of CK7/CK20 in different clinical diagnoses of CUP
The CK7+/CK20- expression pattern accounted for 55.3% of all CUP cases, making it the most common pattern. The primary sites frequently associated with this pattern were: unknown origin (24.9%), lung (22.77%), breast (17.24%), pancreatobiliary system (11.72%), ovary (6.9%), thyroid (4.13%), uterus (3.44%), upper gastrointestinal tract (2.75%), lower gastrointestinal tract (1.37%), bladder (1.37%), prostate (1.37%), liver (0.68%), kidney (0.68%), and squamous cell carcinoma (0.68%).
This was the second most common pattern in the current study, accounting for 19% of all CUP cases. The primary sites frequently associated with this pattern were: prostate (28%), unknown origin (26%), kidney (14%), lung (10%), breast (8%), upper gastrointestinal tract (4%), liver (4%), nasopharynx and squamous cell carcinoma (6%).
CK7+/CK20+ was the third most common pattern, accounting for 15% of all CUP cases. The primary sites frequently associated with this pattern were: unknown origin (38.5%), pancreatobiliary system (23.07%), upper gastrointestinal tract (10.25%), lower gastrointestinal tract (7.69%), bladder (10.25%), lung (5.12%), and ovary (5.12%).
The CK7-/CK20+ pattern was the least common, accounting for 10.7% of all CUP cases. The primary sites frequently associated with this pattern were: lower gastrointestinal tract (60.73%), unknown origin (21.42%), appendix (7.14%), upper gastrointestinal tract (7.14%), and bladder (3.57%).
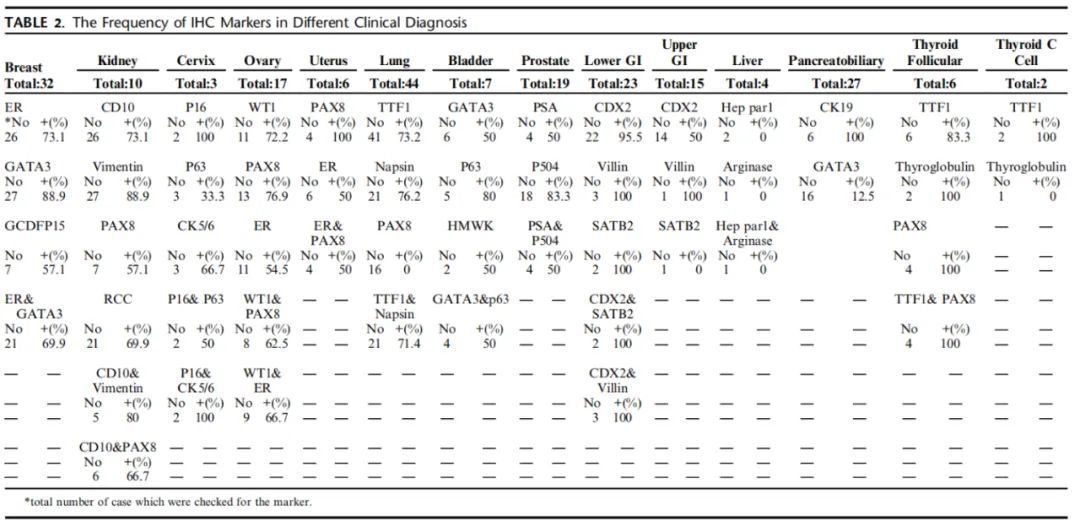
Tables 1 and 2 show the frequencies of different CK7/CK20 patterns and organ-specific IHC markers.
Table 1. Frequency distribution of different CK7/CK20 expression patterns in different primary organs
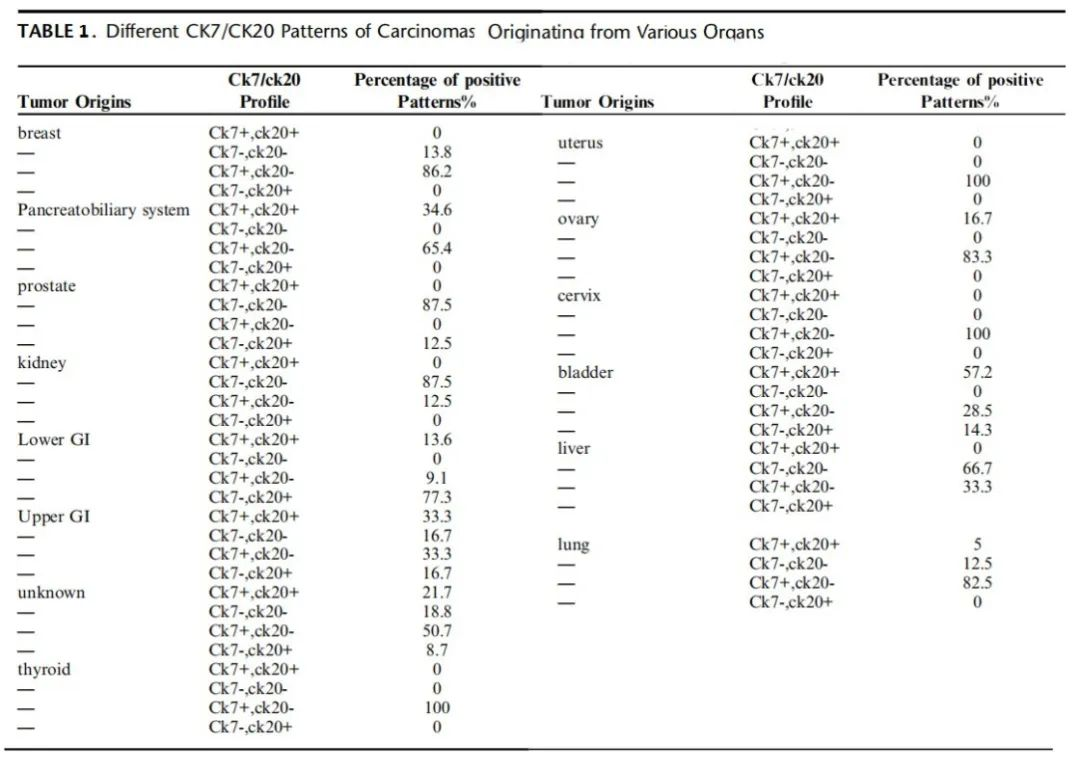
Table 2. Frequency distribution of organ-specific IHC markers in different clinical diagnoses
Figures 3-6 are some examples of primary tumor site identification based on CK7/CK20 staining patterns and organ-specific markers:
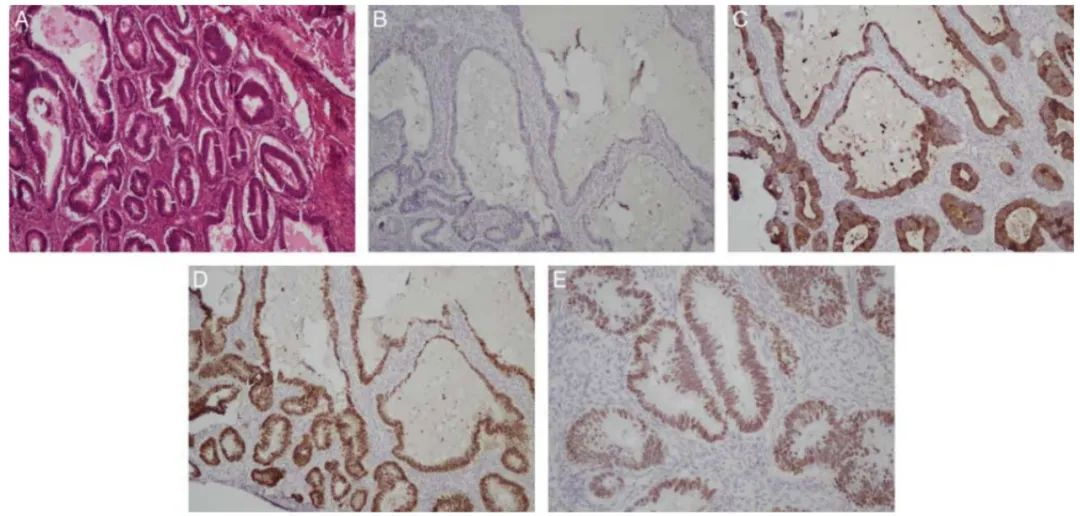
Figure 3. Metastatic carcinoma of lower gastrointestinal tract origin (A, HE 400×; B-E, IHC staining results for CK7, CK20, CDX2, and SATB2: CK7-/CK20+, CDX2+, SATB2+).
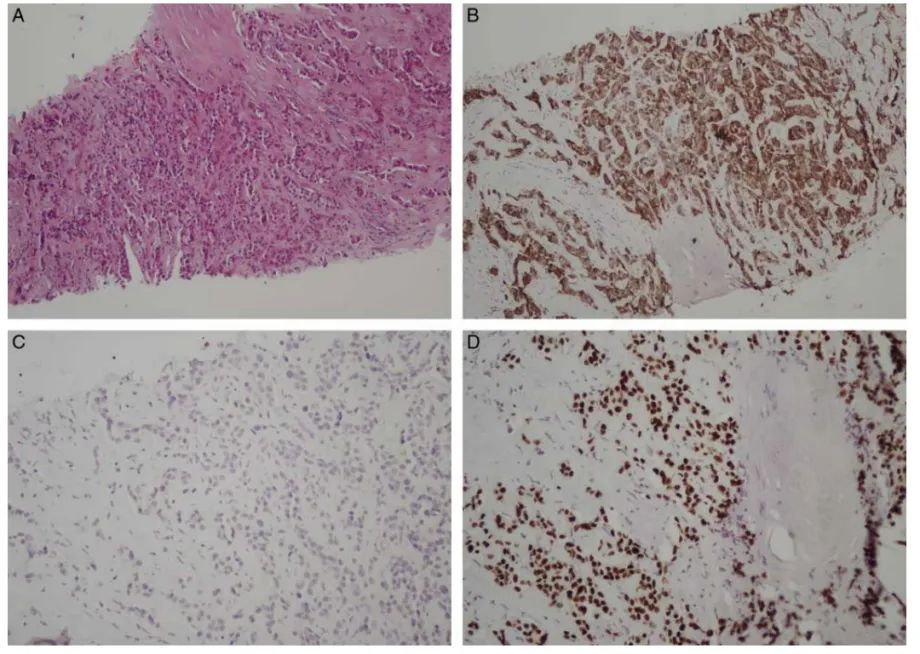
Figure 4. Metastatic carcinoma of breast origin (A, HE 250×; B-D: IHC staining results for CK7, CK20, and GATA3: CK7+/CK20-, GATA3+).
Figure 5. Metastatic carcinoma of kidney origin (A, HE 400×; B-G: IHC staining results for CK, CK7, CK20, Pax-8, vimentin, and CD10: CK7-/CK20-).
Figure 6. Metastatic carcinoma of pancreatobiliary origin (A, HE 250×; B-E: IHC staining results for CK7, CK20, CK19, and CDX2: CK7+/CK20+, CK19+, CDX2-).
All CK7/CK20 expression patterns were detected in cases of gastrointestinal origin. The study showed that CDX2 was positively expressed in 95.5% of lower gastrointestinal tract and 50% of upper gastrointestinal tract origin cases, and in over 90% of colorectal cancers. However, it is not a good predictive marker for metastatic carcinoma of lower gastrointestinal origin because it may be positively expressed in all metastatic carcinomas of gastrointestinal origin, with a positive rate of 18%-70% or more in gastric cancer, and positive in 74% of ovarian metastases from gastric origin. In this study, SATB2 was positively expressed in CUP of lower gastrointestinal origin, showing high sensitivity and specificity for metastatic carcinoma of colorectal origin. Ma et al. demonstrated that SATB2 is a new marker, positively expressed in 85% of primary and metastatic signet-ring cell carcinomas of colorectal origin, but it is not suitable as a marker for metastatic carcinoma of upper gastrointestinal origin.
In this study, Villin was positively expressed in metastatic carcinomas of both upper and lower gastrointestinal origin. Studies show that Villin has a high positive rate in colorectal cancer: 75%-90% or more, especially in well-differentiated cases. Additionally, Villin expression is not limited to gastrointestinal cancers; it is also positively expressed in 40% of pancreatic cancers, 78% of esophageal cancers, and 64% of mucinous ovarian cancers.CDX2, Villin, and SATB2 help identify metastatic carcinomas of lower gastrointestinal origin. For cases possibly of upper gastrointestinal origin, the combined use of Villin and CDX2 can improve diagnostic accuracy.
Four cases were clinically diagnosed as metastatic carcinoma of liver origin but lacked accurate pathological diagnosis. The CK expression patterns were CK7-/CK20- (66.7%) and CK7+/CK20- (33.3%), but Hepatocyte and Arginase-1 were both negative. Studies show that Hepatocyte is positively expressed in 70%-100% of hepatocellular carcinomas, with a sensitivity and specificity of 70% and 84%, respectively. Arginase-1 has a sensitivity of 96% for hepatocellular carcinoma, even in poorly differentiated cases. However, these four cases did not express Hepatocyte or Arginase-1 and should be classified as of undetermined origin.
86.2% and 13.8% of breast origin cases showed CK7+/CK20- and CK7-/CK20- expression patterns, respectively. ER, GATA3, and GCDFP-15 were positively expressed in 73.1%, 88.9%, and 57.1% of breast origin cases, respectively. Studies show that GATA3 has higher sensitivity than GCDFP-15 for breast cancer diagnosis, so the combined use of ER and GATA3 helps diagnose most breast cancers.
CK7-/CK20- was the most prevalent expression pattern for metastatic carcinoma of kidney origin, followed by CK7+/CK20-. CD10, Vimentin, and Pax-8 were positively expressed in over 70% of renal cancers, aiding in identifying kidney origin. Studies show that Pax-8 has a higher positive rate in metastatic carcinomas and is a specific marker for primary and metastatic renal cell carcinoma; CD10 is positively expressed in 91% of clear cell renal cell carcinomas, and Vimentin has 100% sensitivity for clear cell renal cell carcinoma.This study shows that the combined application of Vimentin, Pax-8, and CD10 helps identify metastatic carcinomas of kidney origin.
Metastatic carcinomas of cervical origin commonly express the CK7+/CK20- pattern. All evaluated cases were poorly differentiated, and the type of cervical cancer (i.e., squamous cell carcinoma or adenocarcinoma) could not be determined by histomorphology,therefore, an IHC panel including p16, p63, and CK5/6 was used to diagnose cervical cancer.They are reported to have good sensitivity and specificity for diagnosing cervical squamous cell carcinoma. Wang et al. found that p16 was positively expressed in 98% of cervical squamous cell carcinomas metastatic to the lung.
83.3% of metastatic carcinomas of ovarian origin expressed the CK7+/CK20- pattern, with the remainder being CK7+/CK20+. Among CK7+/CK20- cases, 72.7% were WT1 positive, 6.9% were Pax-8 positive, and 54.5% were ER positive. Studies found that in metastatic carcinomas of ovarian origin, WT1 positivity exceeds 90%, while Pax-8 and ER positivity rates are 70%-99% and 85%-90%, respectively. This study shows that 66.7% of metastatic carcinomas of ovarian origin co-expressed WT1 and Pax-8. Since ovarian serous carcinoma is the most common ovarian epithelial tumor with a high risk of metastasis,therefore, WT1, Pax-8, and ER can serve as a highly sensitive IHC panel for diagnosing metastatic carcinomas of ovarian origin (especially the CK7+/CK20- pattern).When diagnosing CUP with a CK7+/CK20+ pattern, mucinous carcinoma should be considered, and markers like CDX2 may be useful.
All metastatic carcinomas of uterine origin expressed the CK7+/CK20- pattern. Pax-8 and ER were positively expressed in 100% and 50% of cases, respectively. Studies show that 84%-93% of endometrial cancers are Pax-8 positive,therefore, Pax-8 is a useful marker for identifying adenocarcinomas of uterine origin at extrauterine sites.Additionally, Alkushi and Kounelis et al. found ER positivity in 73% and 54% of endometrial cancers, respectively.
82.5% of metastatic carcinomas of lung origin expressed the CK7+/CK20- pattern, 12.5% expressed CK7-/CK20-, and 5% expressed CK7+/CK20+. TTF-1 was positively expressed in 73.2% of cases, consistent with previous studies showing TTF-1 positivity in 70%-100% of various lung cancers, but with lower positivity in poorly differentiated adenocarcinomas.
76.2% of metastatic carcinomas of lung origin were positive for Napsin A. Studies show that Napsin A is positive in over 80% of patients and is more sensitive than TTF-1 in diagnosing metastatic carcinomas of lung origin. Pax-8 was negative in all metastatic carcinomas of lung origin, helping to distinguish lung origin from thyroid origin tumors, as both cancers can be TTF-1 positive.
Studies show that the combined use of TTF-1 and Napsin A has high sensitivity for detecting lung adenocarcinoma. All metastatic carcinomas of thyroid origin expressed the CK7+/CK20- pattern. Among six cases of follicular cell origin, TTF-1 positivity was 83.3%, while Thyroglobulin and Pax-8 positivity were both 100%. Two cases of medullary carcinoma were positive for TTF-1 and Calcitonin but negative for Thyroglobulin, consistent with previous studies: TTF-1 and Pax-8 both show high sensitivity in metastatic carcinomas of thyroid origin. Positive expression of these markers is more common in well-differentiated metastatic carcinomas of thyroid follicular origin (papillary and follicular carcinomas) compared to medullary and anaplastic thyroid carcinomas. On the other hand, Zhang et al. found inconsistency with previous studies: Pax-8 was positive in 31.2% of papillary carcinomas and 40% of follicular carcinomas. Thyroglobulin positivity rates vary between primary thyroid follicular epithelial carcinomas and metastatic sites, ranging from 60%-100%. TTF-1, Thyroglobulin, and Pax-8 as an IHC panel have 100% sensitivity for carcinomas of follicular cell origin. Thyroglobulin, TTF1, and Calcitonin as an IHC panel have high predictive value for carcinomas of C-cell origin.
87.5% of metastatic carcinomas of prostate origin expressed the CK7-/CK20- pattern, with the remainder being CK7-/CK20+. AMACR/p504s and PSA were positively expressed in 83.3% and 50% of cases, respectively. Co-expression of PSA and AMACR/p504s was observed in 50% of cases. Studies show that PSA expression in prostate cancer has high sensitivity and specificity, but its application in metastatic sites is less common, and PSA positivity is higher in well-differentiated prostate cancer compared to high-grade prostate cancer. AMACR/p504s is positively expressed in 80%-100% of prostate cancers, showing high sensitivity.
65.4% of metastatic carcinomas of pancreatobiliary origin expressed the CK7+/CK20- pattern, with the remainder expressing CK7+/CK20+. All patients were positive for CK19, and 12.5% were positive for GATA3. Studies show that CK19 is positively expressed in 100% of liver metastases from pancreatic adenocarcinoma, with 100% sensitivity in pancreatic cancer diagnosis. Pancreatic ductal adenocarcinoma is one of the non-breast cancers with the highest GATA3 positivity rate, with a sensitivity of 37%. Clark et al.’s study showed GATA3 positivity in 10% of pancreatic cancers. Although there is no specific marker for detecting pancreatobiliary carcinoma,CK19 may help diagnose cases of pancreatobiliary system origin.。
It should be noted that the expression of cytoplasmic IHC markers is often influenced by the degree of tumor differentiation. In many cases, markers localized to the cytoplasm, which are associated with tumor cell differentiation and tissue specificity, are easily lost in metastases, while markers localized to the nucleus are least affected. In this study, IHC more easily detected carcinomas originating from the upper and lower gastrointestinal tract, breast, kidney, prostate, ovary, lung, and thyroid compared to those originating from the cervix, pancreatobiliary system, and liver.
|
Antibody Name
|
Product Number
|
Clone Number
|
Cellular Localization
|
|
CK7
|
MAB-0828
|
MX053
|
Cytoplasm
|
|
CK20
|
MAB-0834
|
MX059
|
Cytoplasm
|
|
CDX2
|
RMA-0631
|
EPR2764Y
|
Nucleus
|
|
SATB2
|
RMA-0750
|
EP281
|
Nucleus
|
|
Villin
|
MAB-0540
|
CWWB1
|
Cytoplasm
|
|
Hepatocyte
|
MAB-1034
|
MX119
|
Cytoplasm
|
|
Arginase-1
|
RMA-0806
|
EP261
|
Cytoplasm/Nucleus
|
|
GATA3
|
RMA-1067
|
EP368
|
Nucleus
|
|
GCDFP-15
|
MAB-1035
|
MX120
|
Cytoplasm
|
|
ER
|
Kit-0012
|
SP1
|
Nucleus
|
|
CD10
|
MAB-0668
|
MX002
|
Cytoplasm/Membrane
|
|
Vimentin
|
MAB-0735
|
MX034
|
Cytoplasm
|
|
Pax-8
|
RMA-1024
|
MXR013
|
Nucleus
|
|
p63
|
MAB-0694
|
MX013
|
Nucleus
|
|
CK5/6
|
MAB-0744
|
MX040
|
Cytoplasm
|
|
WT-1
|
MAB-0678
|
MX012
|
Nucleus
|
|
TTF-1
|
MAB-0677
|
MX011
|
Nucleus
|
|
NapsinA
|
MAB-0704
|
MX015
|
Cytoplasm
|
|
Thyroglobulin
|
MAB-0797
|
2H11+6E1
|
Cytoplasm
|
|
Calcitonin
|
RMA-0553
|
SP17
|
Cytoplasm
|
|
AMACR/p504s
|
RMA-1023
|
MXR012
|
Cytoplasm
|
|
PSA
|
MAB-0719
|
MX030
|
Cytoplasm
|
|
CK19
|
MAB-0829
|
MX054
|
Cytoplasm
|
References:
[1] Mokhtari Maral,Safavi Dornaz,Soleimani Neda, et al. Carcinoma of Unknown Primary Origin: Application of Immunohistochemistry With Emphasis to Different Cytokeratin 7 and 20 Staining Patterns[J]. Applied Immunohistochemistry & Molecular Morphology,2022.
For more information, please contact: 800-8581156 or 400-889-9853


