
A Glimpse of the Whole Picture: P16/Ki-67 Dual Staining for More Accurate Cervical Cancer Screening

As is well known, cervical cancer is a major threat to women’s health and life, ranking first among gynecological malignant tumors. The incidence of cervical cancer in China is a “high-risk area” worldwide, with approximately 130,000 new cases annually, accounting for 28% of the world’s new cases.
Moreover, in recent years, there has been a clear trend of younger onset of cervical cancer. Fortunately, cervical cancer is currently the only cancer with a clear cause (persistent HPV infection) that can be prevented and treated early.
Over the past two decades, the prevention and treatment of cervical cancer have also undergone revolutionary changes, from liquid-based cytology, TBS classification, to HPV-DNA testing, and now the popular HPV vaccine.
However, finding a cervical cancer screening strategy suitable for China’s national conditions and carrying out effective standardized diagnosis and treatment of cervical precancerous lesions is extremely important.
Currently, the main methods for cervical cancer screening are:
(1) Cytological screening: Determine whether further HPV testing is needed.
(2) HPV-DNA testing: Determine whether it is a high-risk HPV infection and whether continued cytological testing is necessary.
(3) Cytology combined with HPV-DNA testing: Determine whether it is a 16/18 type HPV infection, whether it is ASCUS or LSIL, and whether colposcopy is needed.
However, through comparison of various screening methods, we found that cytological screening alone has low sensitivity and poor repeatability; HPV testing alone has low specificity and a high colposcopy referral rate, leading to patient anxiety and a certain degree of overtreatment; cytology combined with HPV testing, although effectively controlling the number of colposcopies to some extent, still has a large proportion of ASCUS and LSIL cases where no low-grade or high-grade cervical lesions are found during histological confirmation by colposcopy.
In 2012, CAP/ASCCP jointly issued guidelines, recognizing P16 as the only biomarker with sufficient clinical research data to confirm its use in the diagnosis of cervical precancerous lesions. The guidelines also recommend: For CIN2, CIN3, and other lesions such as atrophy, immature squamous metaplasia, reparative changes, and post-conization, P16 should also be used for differential diagnosis. In 2014, the WHO Classification of Female Genital Tumors (Fourth Edition) proposed that P16 immunohistochemistry can be well used to assess HSIL.
p16 functions to inhibit cell proliferation during the cell cycle arrest phase, while another biomarker, Ki-67, indicates cell proliferation. Therefore, a physiologically normal cell cannot simultaneously express p16 and Ki-67; if both are expressed, it suggests cell cycle dysregulation.
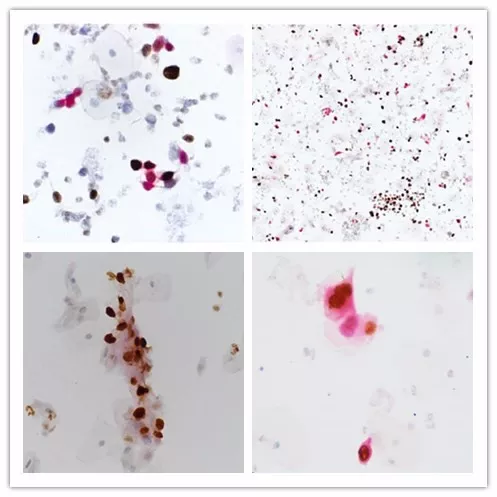
Maxin P16/Ki-67 Dual Staining Image
Maxin independently developed China’s first p16/Ki-67 immunocytochemical dual staining kit, which can simultaneously detect overexpressed p16 and Ki-67 after persistent HPV infection. After staining, if in the same cell, the nucleus appears brown-yellow (Ki-67 positive) and the cytoplasm appears red (p16 positive), it strongly suggests CIN2+ lesions, requiring immediate colposcopy; if dual staining is negative, it indicates a low risk of cancer, and re-examination can be done after one year.
p16/Ki-67 Immunocytochemical Dual Staining Kit Applicable Population
Research confirms that Maxin p16/Ki-67 dual staining detection has high sensitivity and specificity
Wang Hairui et al. conducted liquid-based cytology (TCT) and HR-HPV testing on 980 cervical cancer screening cases, used Maxin p16/Ki-67 dual staining reagent on retained specimens, and compared the results with cervical histopathological findings. The results showed that the sensitivity of p16/Ki-67 dual staining for diagnosing CIN2+ and CIN3+ lesions was 89.3% and 94.1%, respectively, and the specificity was 69.3% and 66.8%, respectively. This is significantly higher than the sensitivity and specificity of TCT.
Another article published in Oncotarget also showed that in the triage of women with negative cytology/HPV positive, Maxin p16/Ki-67 dual staining had a sensitivity of 90.9% for diagnosing CIN2+ and 100% for diagnosing CIN3+. This means that p16/Ki-67 dual staining can detect the vast majority of precancerous lesions while reducing unnecessary colposcopies.

p16/Ki-67 dual staining detection can help doctors objectively determine which populations need further colposcopy, significantly reduce the colposcopy referral rate, avoid overtreatment, and assist clinicians in precise stratified management of patients, thereby achieving early intervention.