Fumarate hydratase (FH), also known as fumarate hydratase, is encoded by a gene located at chromosome 1q42.3-q43, with a sequence length of 510 amino acids. In eukaryotes, it exists as an isomerase: it is present in cells in both cytoplasmic and N-terminal extended forms. The N-terminal extended form is located in mitochondria and participates in the TCA cycle: catalyzing the conversion of fumarate to L-malate. The cytoplasmic form of FH is involved in amino acid and fumarate metabolism and can translocate into the nucleus to participate in DNA damage repair.
2SC is a product of FH loss of function: FH gene defects lead to blockage of the TCA cycle and/or abnormal respiratory chain function, causing accumulation of oxygen free radicals and inducing oxidative stress. Fumarate, acting as an endogenous electrophile, reacts with free thiol groups. Through Michael addition, it forms thioether bonds with cysteine residues in various proteins, ultimately resulting in the formation of 2SC.
Defects in the FH gene cause cells to lose the ability to metabolize fumarate, leading to a series of compensatory metabolic changes such as pseudohypoxia drive, oxidative stress, decreased AMPK levels, and DNA repair inhibition (as shown in Figure 1). These changes trigger carcinogenic transformations, causing various diseases including hereditary leiomyomatosis and renal cell carcinoma (HLRCC) syndrome, paraganglioma, pheochromocytoma, Leydig cell tumor, ovarian cystadenoma, and others.
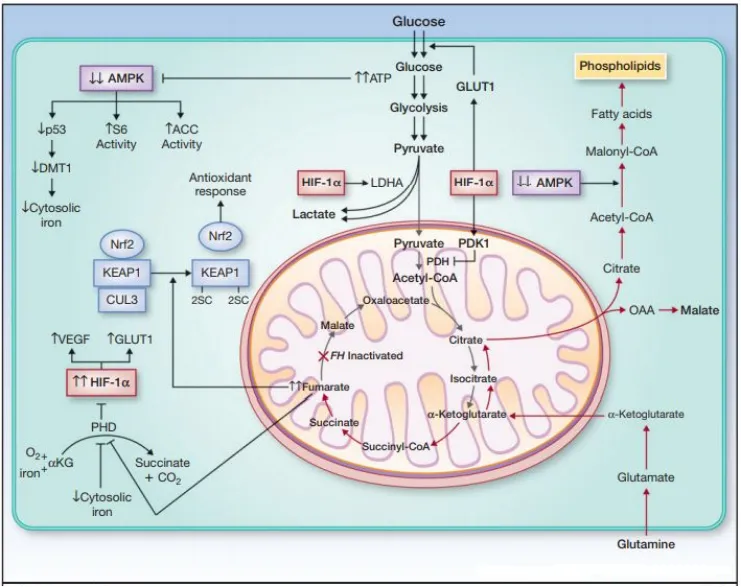
Figure 1. Pathogenic mechanism of FH deletion or mutation
Among these, HLRCC has a severe disease course and poor prognosis. Its clinical manifestations include FH-deficient cutaneous and/or uterine leiomyomas and renal cell carcinoma, with their respective characteristics as follows:
Cutaneous leiomyoma is the most sensitive and specific clinical hallmark symptom in HLRCC patients. It presents as flesh-colored or reddish-brown papules or nodules, often multiple on the limbs, and is frequently painful, triggered by cold, heat, or touch. Prevalence increases with age, often appearing in the teenage years, but can also occur in childhood. There is no definitive unique morphological appearance.
Uterine leiomyoma is usually the primary manifestation in female HLRCC patients. Affected patients typically develop symptomatic leiomyomas at an earlier age, often requiring early surgical intervention. Morphologically, features include staghorn vessels, eosinophilic cytoplasmic globules, and large, eosinophilic nucleoli. When these features appear within a tumor, the possibility of an FH-deficient tumor should be considered, especially in younger patients.
FH-deficient renal cell carcinoma mostly occurs in the context of HLRCC, but sporadic cases can also arise due to loss of function in both FH alleles. It often presents as a solitary mass in one kidney, with a large tumor size and strong invasiveness, typically being a major cause of patient mortality. Morphologically, it is highly heterogeneous, often exhibiting various structural features such as cribriform, tubular-cystic, tubular-papillary, and nested patterns.
Diagnostic Value of FH and 2SC in FH-deficient Tumors
In pathological diagnosis, preliminary morphological screening lacks sensitivity and specificity for FH-deficient tumors. Studies by Miettinen et al. showed that in the diagnosis of uterine leiomyomas, features like eosinophilic nucleoli with perinucleolar halos, eosinophilic hyaline globules, and staghorn vessels can appear in approximately 69%, 19%, and 39% of uterine leiomyomas without FH deletion, respectively. In renal cell carcinoma diagnosis, due to morphological overlap with various types of renal tumors, diagnosing this type of renal cancer is often challenging. It has frequently been diagnosed as type II papillary renal cell carcinoma, collecting duct carcinoma, or tubulocystic carcinoma in the past. Therefore, further IHC testing is required.
Common IHC testing involves FH-negative screening. However, studies by XiuYi Pan et al. also found that some cases with FH gene mutations still show positive or weakly positive FH expression, indicating that not all FH-deficient cases exhibit loss of FH staining. Staining with a single FH antibody lacks certain sensitivity. 2SC, as a product of FH loss of function, can compensate for the sensitivity defect of FH staining through its positive expression in cells. Therefore, FH loss and 2SC overexpression can serve as immunohistochemical markers for diagnosing and screening tumors caused by FH deletion or mutation. Combined detection of both can enhance the potential of IHC for detecting FH-deficient diseases.
Related studies by Joseph N M and Chen Y B et al. show that the immunophenotypic pattern of FH-negative/2SC-positive has high consistency with the results of molecular biological techniques detecting germline or somatic mutations of the FH gene in tumor tissues. It demonstrates good sensitivity and specificity for detecting FH-deficient leiomyomas and uterine leiomyomas and can effectively distinguish FH-deficient renal cell carcinoma from diseases like type II papillary renal cell carcinoma, collecting duct carcinoma, or tubulocystic carcinoma. Therefore, combined IHC detection of 2SC and FH can greatly facilitate the diagnosis of HLRCC.
Furthermore, the combination of FH-negative/2SC-positive can also be used for detecting diseases such as paraganglioma, pheochromocytoma, Leydig cell tumor, ovarian cystadenoma, etc.
Related Antibodies from Maixin
|
Antibody Name
|
Product Number
|
Clone Number
|
Cellular Localization
|
|
FH
|
MAB-1014
|
J-13
|
Cytoplasm
|
|
2SC
|
RAB-1015
|
Rabbit Polyclonal
|
Cytoplasm/Nucleus
|
[1] Zhao Zichen, Wang Wenhui, Feng Fengzhi. Research Progress on Hereditary Leiomyomatosis and Renal Cell Carcinoma Syndrome[J]. Journal of Practical Obstetrics and Gynecology, 2018, v.34(04):23-26.
[2] Zhang Wei, Chu Jing, Zou Yuwei, et al. Clinicopathological Features of Fumarate Hydratase-deficient Renal Cell Carcinoma[J]. Chinese Journal of Pathology, 2019, 048(002):120-126
[3]Zyla Roman E,Hodgson Anjelica. Gene of the month: FH.[J]. Journal of clinical pathology,2021:1-5
[4]Pan X , Zhang M , Yao J , et al. Fumaratehydratase-deficient renal cell carcinoma: a clinicopathological and molecular study of 13 cases[J]. Journal of Clinical Pathology, 2019, 72(11):jclinpath-2019-205924.
[4] Miettinen M,Felisiak-Golabek A,Wasag B,et al. Fumarase-deficient uterine leiomyomas: an immunohistochemical,molecular genetic,and clinicopathologic study of 86 cases[J]. Am J Surg Pathol,2016,40( 12) : 1661-1669.
[5] Joseph N M, Solomon D A, Frizzell N, et al. Morphology and Immunohistochemistry for 2SC and FH Aid in Detection of Fumarate Hydratase Gene Aberrations in Uterine Leiomyomas From Young Patients[J]. American Journal of Surgical Pathology, 2015, 39(11):1529-1539.
[6] Chen Y B , Brannon A R , Toubaji A , et al. Hereditary Leiomyomatosis and Renal Cell Carcinoma Syndrome–associated Renal Cancer: Recognition of the Syndrome by Pathologic Features and the Utility of Detecting Aberrant Succination by Immunohistochemistry[J]. The American Journal of Surgical Pathology, 2014, 38(5):627-637

