Pituitary-specific transcription factorsT-PIT (transcription factor 19), also known as TBX19, is a specific transcription factor for the proopiomelanocortin (POMC) lineage and corticotroph cell differentiation. In the 2017 WHO new classification of pituitary tumors, pituitary adenomas are divided into three categories based on the differentiation lineage (origin) of the tumor cells: acidophilic lineage, corticotroph cell lineage, and gonadotroph cell lineage. T-PIT is an important transcription factor for the corticotroph cell lineage, crucial for the differentiation and maturation of its lineage cells. According to this principle, all corticotroph adenomas should be T-PIT positive. If the result is negative and hormone immunohistochemistry is also negative, they are classified as null cell adenomas in the new classification. Similarly, non-functioning pituitary adenomas that are ACTH negative but T-PIT positive are reclassified as silent corticotroph adenomas (SCAs).
Differential diagnosis of silent corticotroph adenomas
SCAs clinically present as non-functioning adenomas, with some showing ACTH immunopositivity but lacking biochemical and clinical manifestations of hypercortisolism. After the new classification added pituitary-restricted transcription factors, tumors with positive T-PIT immunostaining were reclassified as SCAs. Among 119 hormone-negative null cell adenomas, re-evaluation with ACTH and T-PIT immunohistochemical staining led to 30% of the tumors being re-identified as SCAs. In another large cohort of 814 pituitary adenomas, re-testing with hormones and transcription factors revealed that only 4.8% were confirmed as SCAs. SCAs are also a type of refractory pituitary tumor, with tumor size and invasiveness similar to silent gonadotroph adenomas, but the former is more invasive and has a tendency to recur.
Differential diagnosis of null cell adenomas
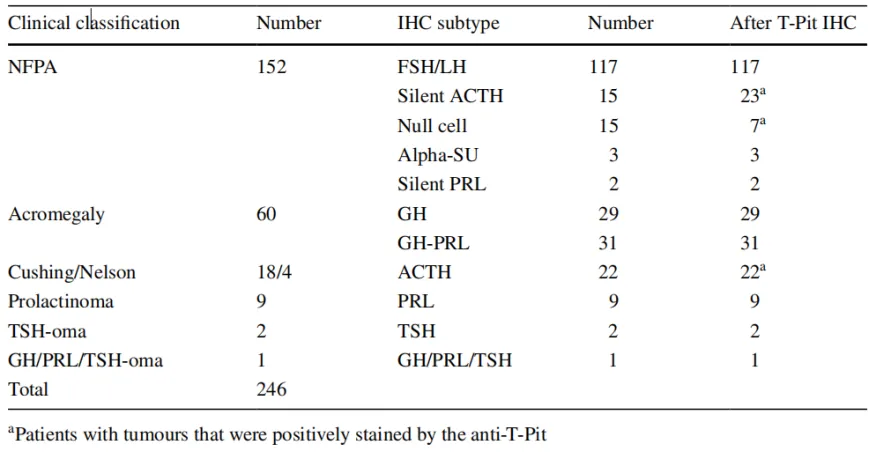
In a cohort of 251 pituitary adenomas, 56 patients were studied. Using transcription factor analysis, the incidence of null cell adenomas was reduced from 16.3% to 3.2%. Sjöstedt et al. performed IHC staining on 246 pituitary adenoma tissues of different types (Table 1). The results showed that all corticotroph adenomas (silent, primary, and bone metastatic tumors) and 8 out of 15 tumors diagnosed as null cell adenomas were T-PIT positive. All tumors negative for SF-1, PIT-1, or pituitary hormones (except ACTH) were T-PIT positive (1c). Based on immunohistochemical results for hormones and pituitary-specific transcription factors, 97.2% of pituitary tumor patients (239 cases) could be accurately classified into the three lineages: SF-1, PIT-1, and T-PIT. Only 7 remaining cases (2.8%) were re-diagnosed as null cell adenomas.
Table 1. Classification overview of 246 pituitary tumor tissue samples
(Click to view larger image)
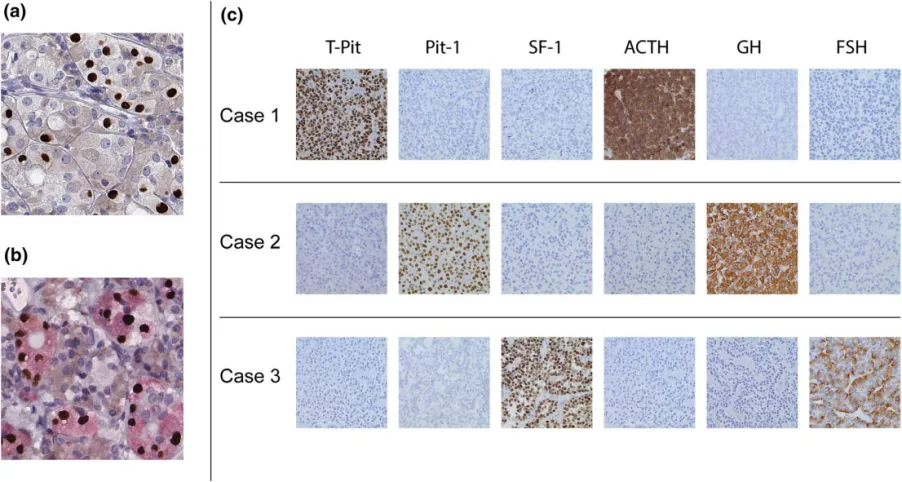
Figure 1. Immunohistochemical staining of hormones and transcription factors in normal adenohypophysis tissue and pituitary tumors; a: T-PIT nuclear staining in adenohypophyseal cells; b: ACTH/T-PIT double staining in adenohypophyseal cells; c: Staining results of pituitary adenoma cases developing towards the three lineages respectively;
Important clinical significance of T-PIT
-
Accurate classification of pituitary tumors, especially those with weak or no hormone expression;
-
Differential diagnosis between silent corticotroph adenomas and null cell adenomas;
-
Identification of potential corticotroph cell differentiation in non-pituitary adenomas;
-
Reducing the cost of immunohistochemical testing for pituitary tumors;
Although pituitary hormone immunohistochemistry is the main basis for diagnosis in most pituitary tumors, the European Pituitary Pathology Group experts reported that approximately 15-20% of pituitary adenomas have limited/absent/abnormal hormone expression. In such cases, analysis of specific transcription factors is crucial for determining pituitary cell lineage differentiation. MXB’s self-developed T-PIT antibody (MX102) has been tested on normal human tissues and various types of pituitary tumors. This antibody is highly specific and exhibits high sensitivity for immunohistochemical detection of cells based on corticotroph differentiation.
|
Antibody Name
|
Product Number
|
Clone Number
|
Cellular Localization
|
|
T-PIT*
|
MAB-0897
|
MX102
|
Nucleus
|
*Indicates MXB clone product
References:
【1】Sjöstedt, E., Bollerslev, J., Mulder, J. et al. A specific antibody to detect transcription factor T-Pit: a reliable marker of corticotroph cell differentiation and a tool to improve the classification of pituitary neuroendocrine tumours. Acta Neuropathol 134, 675–677 (2017). https://doi.org/10.1007/s00401-017-1768-9
【2】Iulia Florentina Burcea,Valeria-Nicoleta Năstase, Cătălina Poiană. Pituitary transcription factors in the immunohistochemical and molecular diagnosis of pituitary tumours — a systematic review.Endokrynologia Polska. Volume/Tom 72; Number/Numer 1/2021. DOI: 10.5603/EP.a2020.0090
For more information, please contact: 800-8581156 or 400-889-9853