
Seventh Issue of “Mai Mai” Pathology Weekly Reading Notes | Immunohistochemical Markers for Respiratory Tract and Lung Tumors
Preface:
We have previously compiled and introduced knowledge points on common epithelial markers in immunohistochemistry. In clinical practice, immunohistochemistry for epithelial tumors in different organs and of various types has certain special characteristics beyond conventional epithelial markers, such as organ-specific markers. Starting from this issue, we will compile and introduce the immunohistochemical features of different organs and tumor types.
Immunohistochemical Markers for Respiratory Tract and Lung Tumors
-
Immunohistochemical markers used for the diagnosis of upper respiratory tract tumors, such as certain CKs, CD56, Syn, CgA, EBV, NUT, p16;
-
Immunohistochemical markers used for the diagnosis of pulmonary epithelial tumors, such as certain CKs, TTF-1, napsin A, p63, p40, CD56, surfactant proteins;
-
Immunohistochemical markers used for the diagnosis of pulmonary mesenchymal tumors, such as CD1a, langerin (CD207), HMB45, STAT6, CD31, CD34, CD99.
TTF-1
The Chinese name for TTF-1 is Thyroid Transcription Factor-1, also known as NKX2-1. Its function is to regulate the development, differentiation, and gene expression of the thyroid, and it also plays a regulatory role in the development and transcriptional activity of the lung and central nervous system (diencephalon). It should be noted that in normal adult thyroid, TTF-1 is expressed in both follicular cells and parafollicular cells (C cells); in normal lung tissue, TTF-1 is strongly positive in type II alveolar epithelial cells and Clara cells of bronchioles, with slightly lower expression in tracheal mucosa.
In routine immunohistochemical detection, TTF-1 is widely used as a sensitive and specific marker for most pulmonary bronchial adenocarcinomas, pulmonary small cell carcinomas, thyroid follicular carcinomas, papillary carcinomas, and medullary carcinomas, with reduced expression in pulmonary large cell carcinomas and thyroid anaplastic carcinomas. Pulmonary squamous cell carcinomas are generally negative, although it has been reported that certain clones such as SPT24 show low-level expression in a minority of pulmonary squamous cell carcinomas.

Figure 1. Strong nuclear positive expression of TTF-1 in pulmonary small cell carcinoma.
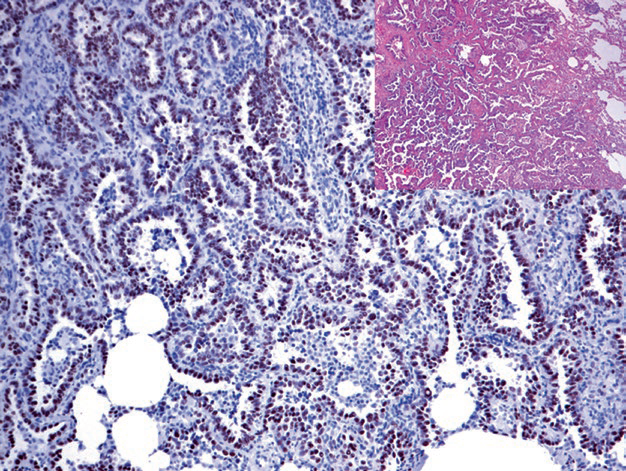
Figure 2. Strong nuclear positive expression of TTF-1 in pulmonary adenocarcinoma.
Positive expression pattern: Nuclear
Recommended positive control tissue: Thyroid
Napsin A
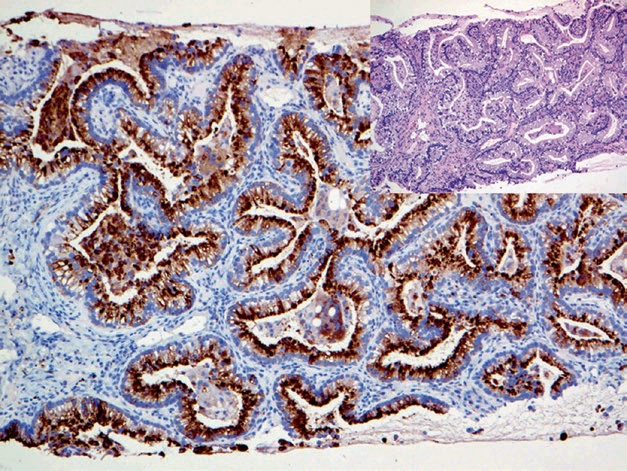
Figure 3. Metastatic pulmonary adenocarcinoma, immunohistochemistry shows strong cytoplasmic positive expression of Napsin A.
Positive expression pattern: Cytoplasmic
Recommended positive control tissue: Lung tissue
Surfactant Proteins
Positive expression pattern: Cytoplasmic
Recommended positive control tissue: Lung tissue
Nuclear Protein in Testis

Table 1. Key Points of Immunohistochemistry for Differential Diagnosis of Upper Respiratory Tract Tumors
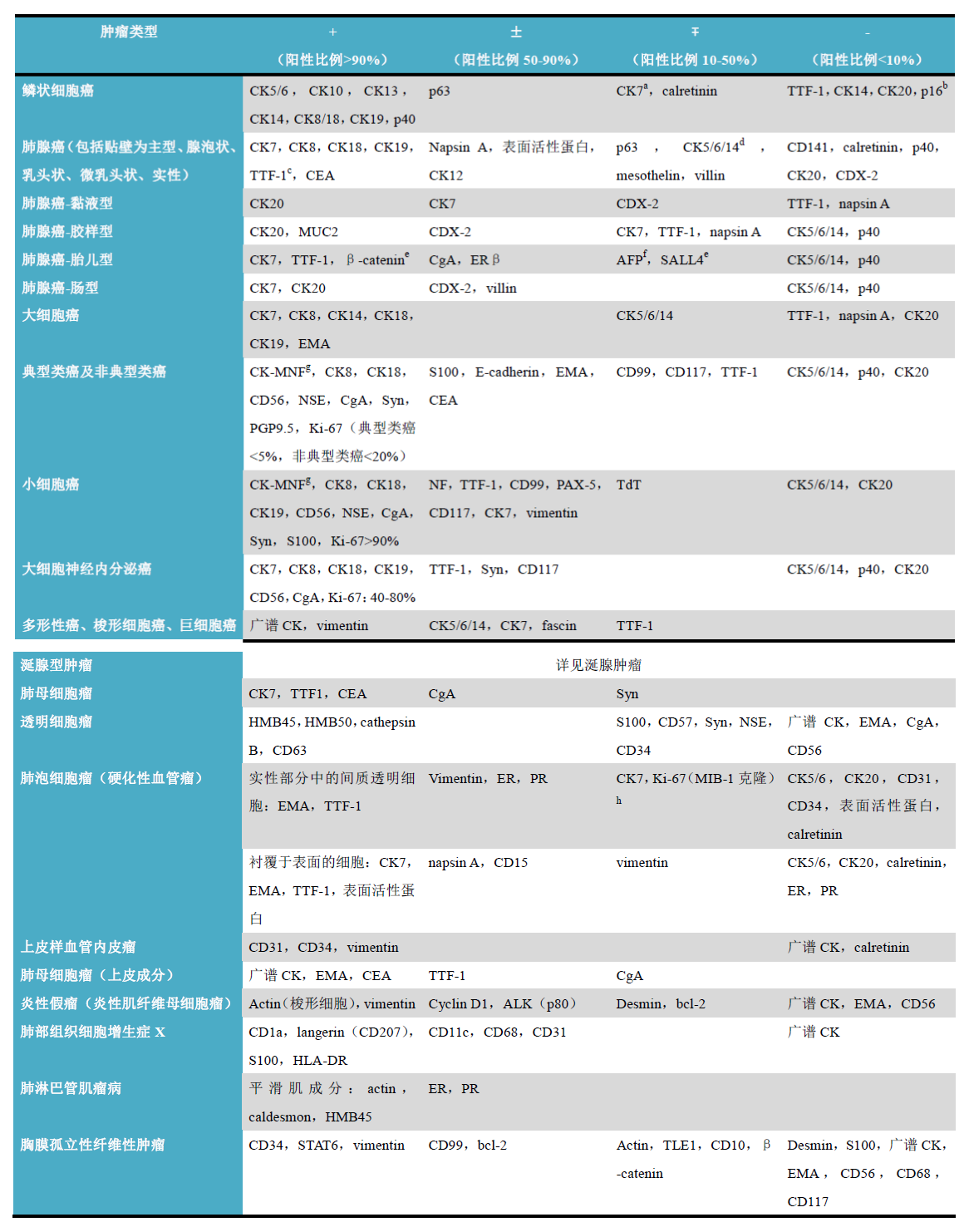
Table 2. Key Points of Immunohistochemistry for Differential Diagnosis of Lung Tumors
Notes for Table 2
-
In pulmonary squamous cell carcinoma, up to 30% may show CK7 positive expression; therefore, when classifying lung cancer, attention should be paid to adding a panel of markers such as TTF-1, Napsin A, p40;
-
p16 can be used to differentiate between primary pulmonary squamous cell carcinoma (negative) and metastatic oropharyngeal squamous cell carcinoma (mostly positive due to HPV infection);
-
Poorly differentiated pulmonary adenocarcinoma may show loss of TTF-1 expression;
-
Often positive in poorly differentiated pulmonary adenocarcinoma;
-
Nuclear positive;
-
Generally seen in poorly differentiated carcinomas;
-
Often shows comma-shaped staining;
-
If the antibody clone used is MIB-1, atypical cell membrane and cytoplasmic staining may be seen.
1
MaiXin: Different clones of the same antibodyhave differences in sensitivity and positive expression. For example, TTF-1 with clone numbers “MX011” or “SPT24” has higher sensitivity in tumors of lung and thyroid origin compared to “8G7G3/1”“, with cell localization being nuclear for both; but “8G7G3/1” can show unique cytoplasmic positive expression in hepatocytes and hepatocellular tumors, while “MX011” and “SPT24” do not exhibit this phenomenon,thereforeinthe differential diagnosis of tumors, the selection of immunohistochemical antibody clones is also very important。
|
Antibody Name |
Clone Number |
Positive Control |
Positive Location |
|
TTF-1* |
MX011 |
Lung adenocarcinoma, Thyroid |
Nuclear |
|
TTF-1 |
SPT24 |
Lung adenocarcinoma, Thyroid |
Nuclear |
|
TTF-1 |
8G7G3/1 |
Lung adenocarcinoma, Thyroid |
Nuclear |
|
Nasin A* |
MX015 |
Lung adenocarcinoma | Cytoplasmic |
*Marked as MaiXin clone products
For more information, please contact: 800-8581156 or 400-889-9853