Immunohistochemical Markers for Diagnosing Epithelial Tumors
Cytokeratins (CK) belong to intermediate filament proteins, which function to form the cytoskeleton and are the most important markers in the diagnosis of epithelial tumors.
In immunohistochemical detection, CK generally shows diffuse cytoplasmic staining, but there are other staining patterns, such as perinuclear and dot-like expression in neuroendocrine tumors. Common tumor types exhibiting this staining pattern also include: Merkel cell carcinoma (perinuclear staining, mainly CK20), small cell carcinoma (mainly CK19), carcinoid and pancreatic endocrine tumors, renal oncocytoma (low molecular weight CK), medullary thyroid carcinoma, seminoma (low molecular weight CK), granular cell tumor, rhabdomyomatous tumors, and a few stromal tumors (such as desmoplastic small round cell tumor, leiomyosarcoma, monophasic synovial sarcoma).
There are many types of CK, broadly divided into two groups: basic CKs, including CK1-8; acidic CKs, including CK9-20. Different CKs are expressed in different epithelial types and at different differentiation stages; and even when different epithelia form tumors, they generally retain their inherent CK expression, which is the theoretical basis for using CK in diagnosis and differential diagnosis. In practice, different CKs from the two groups are often combined for application, such as CK8/18.
Issues with Broad-Spectrum CK
In daily applications, different CKs are often combined into “broad-spectrum” CK or “cocktail” CK for “screening” related to epithelial differentiation or epithelial tumors. Although this approach is very effective, it should be noted that no combination of “broad-spectrum” CK can include all CK types. The more widely used broad-spectrum CK combinations or clone numbers and their specific application ranges are detailed below:
-
AE1/AE3: This combination is a mixture of AE1 and AE3, where AE1 is an acidic CK and AE3 is a basic CK. This combination is widely used but does not react with CK18. A very small number of epithelial tumors are negative or weakly positive for this combination, such as hepatocellular carcinoma, renal cell carcinoma, adrenal cortical carcinoma, prostatic adenocarcinoma, and neuroendocrine tumors. Additionally, it has been reported that this combination cross-reacts with GFAP, which may lead to related misjudgments.
-
KL1: This clone can react with CK1/2/5/6/7/8/11/14/16/17/18, thus it can be considered the most broad-spectrum epithelial marker. However, this clone also cross-reacts with GFAP.
-
MNF116: This clone can react with CK5/6/8/17/19.
-
CAM5.2: This clone can react with CK8/18/19.
-
MAK-6: This clone can react with CK14/15/16/18/19.
-
OSCAR: This broad-spectrum CK can react with CK7/8/18/19, and most epithelial cells and carcinomas derived from such cells are positive. Although this broad-spectrum CK does not cross-react with GFAP, it can react with follicular dendritic cells in lymphoid tissue.
Figure 1. In diffuse gastric adenocarcinoma, tumor cells diffusely express broad-spectrum CK (MNF116).
Recommended quality control for broad-spectrum CK and CK combinations: appendix, tonsil.
Pitfalls in the application of broad-spectrum CK:Certain CKs can be expressed in various non-epithelial tissues and related tumors, as well as tumors with epithelial differentiation, specifically:Mesothelial cells and mesothelioma, smooth muscle and smooth muscle tumors, meningioma and chordoma, epithelioid sarcoma, synovial sarcoma, desmoplastic small round cell tumor, angiosarcoma, a few alveolar rhabdomyosarcomas, clear cell sarcoma, some germ cell tumors, nerve sheath tumors, rhabdoid tumor, malignant melanoma, undifferentiated pleomorphic sarcoma, proliferating myofibroblasts, anaplastic and diffuse large cell lymphoma, plasma cell tumors.
CK-positive expression in mesenchymal tumors is generally focal staining but can also be dot-like. Making a diagnosis of carcinoma based solely on broad-spectrum CK positivity is one of the serious errors in tumor pathological diagnosis. Therefore, in practice, it is essential to pay attention to which specific CKs are positive in the relevant tumor and accordingly select tissue-specific related markers for differentiation.
Benign ectopic epithelial structures within lymph nodes should be carefully noted to avoid misdiagnosis as metastatic carcinoma or tumor cell dissemination, such as ectopic ducts and glandular components in cervical, thoracic, and abdominal lymph nodes, and Müllerian epithelial inclusions and endometriosis in pelvic lymph nodes.
Brief Introduction to Some CKs
CK5 is the main component of the cytoskeleton in basal cells of stratified epithelium; CK6 has the same tissue distribution as CK5 and is generally used in combination with CK5; CK14 generally forms heterodimers with CK5. This marker is an excellent marker for diagnosing squamous cell carcinoma. Combined with CK5, it can effectively mark myoepithelial cells in breast biopsy specimens and basal cells in prostate biopsy specimens.
Recommended positive control tissue: tonsil.
CK5, CK6, and CK14 are expressed in stratified squamous epithelium, myoepithelium, and mesothelium, respectively. Therefore, combinations of these markers can be used for the diagnosis of squamous cell carcinoma and can clearly mark normal myoepithelial cells and myoepithelial components in some tumors (such as salivary gland tumors, myoepithelial tumors). The commonly used 34βE12 combination includes CK1/5/10/14.
The above characteristics are crucial for certain differential diagnoses: in prostate biopsies, basal cells are absent around neoplastic glands; in breast biopsies, myoepithelial and luminal epithelial cells express CK5/6/14 and CK8/18, respectively, which is crucial in differentiating usual ductal hyperplasia, atypical hyperplasia, and ductal carcinoma in situ. However, mesothelial cells also express CK5/6/14, so in abdominal or thymic biopsies and cytology specimens, this group of markers is not suitable for differentiating squamous cell carcinoma from mesothelioma.
Figure 2. In pleural effusion specimens, mesothelioma cells are CK5 positive.
This group of markers is generally not expressed in gastrointestinal adenocarcinomas, germ cell tumors, prostate cancer, thyroid tumors, hepatocellular carcinoma, and renal cell carcinoma.
In recent studies, the combination of CK5/14 has generally been replaced by p63 and p40, as the latter are often expressed in the nuclei of myoepithelial cells and basal cells of glands, as well as in basal and intermediate cells of squamous and urothelial epithelium.
CK7 is expressed in most ductal and glandular epithelium as well as transitional epithelium of the urethra. CK7 is one of the main markers for differential diagnosis of adenocarcinomas of different origins, so it cannot be used alone to distinguish between primary and metastatic adenocarcinomas; CK7 is strongly positive in mesothelial cells, so it is not suitable for differentiating adenocarcinoma from mesothelioma.
Application pitfalls: When differentiating adenocarcinoma from squamous cell carcinoma, it is important to remember that a small number of CK7-positive cells can be present in squamous cell carcinomas of certain sites, specifically the head and neck, lung, esophagus, and cervix, mainly in poorly differentiated carcinomas. CK7 can also be expressed in non-epithelial tumors, such as the epithelioid component of synovial sarcoma. Seminoma, yolk sac tumor, prostate cancer, and pituitary tumors generally do not express CK7.
CK20 is an intermediate filament protein and the main protein in mature intestinal epithelial cells and gastrointestinal mucosal goblet cells. Colorectal adenocarcinoma and ovarian mucinous carcinoma are always CK20 positive, while the positive rate is lower in transitional cell carcinoma. In Merkel cell carcinoma, CK20 shows perinuclear dot-like positivity.
Figure 3. In Merkel cell carcinoma, CK20 shows characteristic perinuclear dot-like staining.
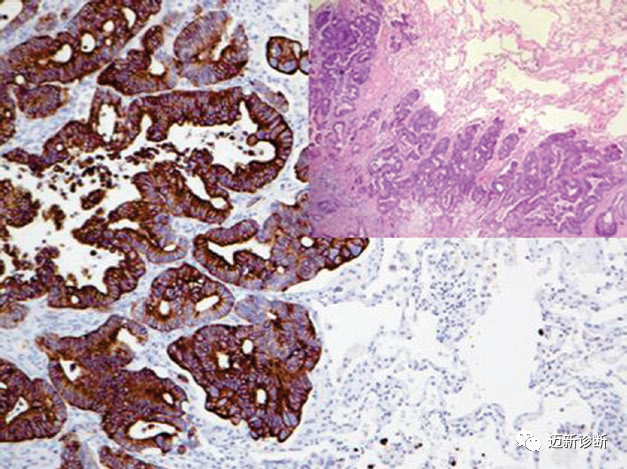
Figure 4. Metastatic colorectal adenocarcinoma strongly expresses CK20.
CK20 is very useful in differentiating reactive atypia from dysplasia in the urinary tract: in normal and reactive transitional epithelium, CK20 expression is limited to umbrella cells; in carcinoma in situ, the entire epithelium expresses it. Squamous cell carcinoma, breast cancer, prostate cancer, thyroid cancer, endometrial adenocarcinoma, and mesothelioma are always CK20 negative.
Since only some carcinomas are CK20 positive, this marker helps differentiate between different types of carcinoma. Combined with CK7, it is an important means to distinguish different types of carcinoma, as detailed earlier.
Recommended positive control tissue:Appendix.
CK8:Generally forms heterodimers with CK18. Both CK8 and CK18 are intermediate filament proteins, expressed early in embryonic development and persist in adult simple epithelium. CK8 is generally expressed in non-squamous cell carcinomas, so it cannot be used to differentiate adenocarcinoma from carcinoid. A few mesenchymal tumors can also express CK8, such as smooth muscle tumors and malignant rhabdoid tumors.
Recommended positive control tissue: appendix.
CK10:Intermediate filament protein, generally related to CK1. CK10 is expressed in keratinized and non-keratinized squamous epithelium. In daily work, CK10 is combined with CK13 and CK14 in a cocktail antibody for marking squamous cell carcinoma.
Recommended positive control tissue: tonsil.
CK13:Expressed in parabasal and intermediate cells of stratified squamous epithelium. Generally combined with CK10 or CK14 in a cocktail antibody, used as a marker for squamous cell carcinoma.
Recommended positive control tissue: tonsil.
CK18:This marker is an intermediate filament protein expressed in simple epithelial cells, seen in most non-squamous cell carcinomas, such as adenocarcinoma of unknown origin, neuroendocrine carcinoma, hepatocellular carcinoma, renal cell carcinoma. Endothelial cells of lymphatic vessels and small veins also express CK18. When using broad-spectrum CK or cocktail combinations, the immunohistochemical appearance may resemble intravascular tumor thrombus. CK18 can also be expressed in smooth muscle cells and smooth muscle tumors.
Recommended positive control tissue: appendix.
CK19:The smallest molecular weight CK, expressed in both simple and stratified epithelium. Most carcinomas are positive, so its role in specific carcinoma classification is limited. Thyroid papillary carcinoma is strongly positive for CK19, which can be combined with other markers such as CD56 to differentiate thyroid papillary carcinoma from thyroid follicular carcinoma, the latter generally being negative or weakly positive for CK19.
Recommended positive control tissue: appendix.
Mai Mai: The CK series antibodies are numerous and have varied uses! It is worth mentioning that the current domestic CK antibody clones from Mai Xin seriesperform excellently and have received praise from many pathology teachers!
|
Antibody Name
|
Product Number
|
Clone Number
|
Positive Location
|
|
CK5&6
|
MAB-0744
|
MX040
|
Cytoplasmic
|
|
CK7
|
MAB-0828
|
MX053
|
Cytoplasmic
|
|
CK8
|
MAB-0670
|
MX004
|
Cytoplasmic |
| CK8&18 |
MAB-1002
|
MX004+MX035
|
Cytoplasmic |
|
CK14
|
MAB-0832 |
MX057 |
Cytoplasmic |
| CK17 |
MAB-0833 |
MX058 |
Cytoplasmic
|
| CK18 |
MAB-0737
|
MX035 |
Cytoplasmic |
CK19
|
MAB-0829 |
MX054
|
Cytoplasmic |
CK20
|
MAB-0834 |
MX059
|
Cytoplasmic |
CK(PAN)
|
MAB-0671 |
MX005
|
Cytoplasmic |
