
Pathology Weekly Reading Notes by “Mai Mai” | Issue 2
Preface:
In the previous article, based on the book “Immunohistochemistry in Tumor Diagnostics,” we briefly introduced some common issues in immunohistochemistry, such as the staining patterns of immunohistochemical markers; and introduced the time-saving, cost-effective, and highly instructive immunohistochemical panels proposed in the book for tumor lesions with no clear morphological direction or uncertain tissue differentiation.
If morphology suggests a direction of differentiation, corresponding tissue-specific markers can be added to assist in diagnosis, or further related tests can be performed based on the preliminary immunohistochemical results from the aforementioned panels.Today’s content is primarily a presentation of pure, practical information addressing this issue.
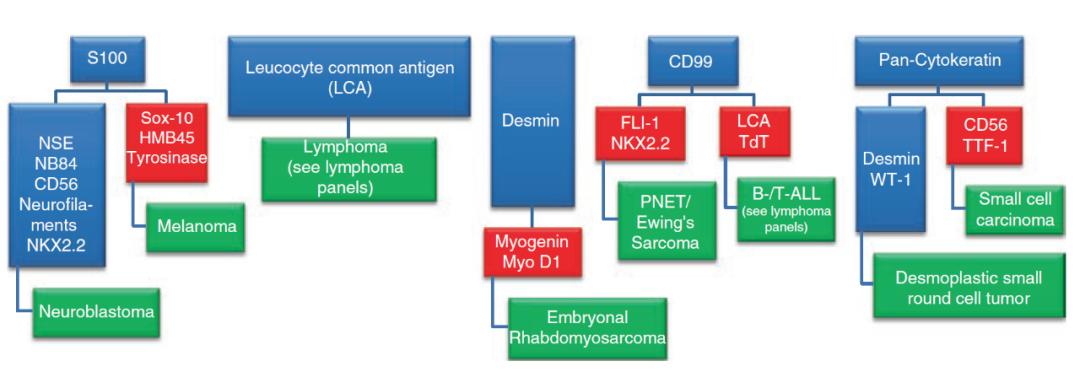
Figure 1. Immunohistochemical diagnostic approach for tumors with small blue round cell morphology.
Detailed Explanation of Figure 1
-
If S100 is positive, other markers should be considered in combination:If NSA, NB84, CD56, NF, NKX2.2 are positive, neuroblastoma should be considered;If SOX-10, HMB45, and tyrosinase are positive, malignant melanoma should be considered;
-
If LCA is positive, lymphoma is often considered; more details will be discussed later;
-
If desmin is positive, and myogenin, MyoD1 are positive, then embryonal rhabdomyosarcoma should be considered;
-
If CD99 is positive, and FLI-1, NKX2.2 are positive, then PNET/Ewing sarcoma should be considered; if LCA, TdT are positive, then B-cell or T-cell acute lymphoblastic leukemia should be considered;
-
If broad-spectrum CK is positive, and desmin, WT-1 are positive, then desmoplastic small round cell tumor should be considered; if CD56, TTF-1 are positive, then small cell carcinoma should be considered.
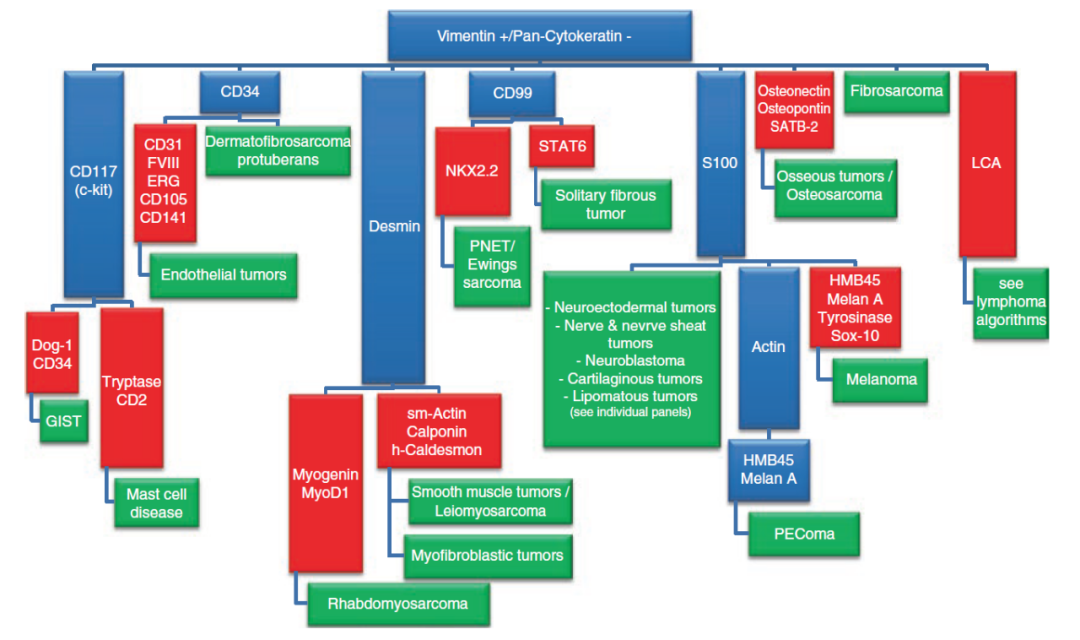
Figure 2. Immunohistochemical diagnostic approach for tumors positive for Vimentin and negative for broad-spectrum CK.
Detailed Explanation of Figure 2
-
If CD117 is positive, and Dog-1, CD34 are positive, it supports GIST; if tyrosinase, CD2 are positive, mast cell disease should be considered;
-
If CD34 is positive, dermatofibrosarcoma protuberans should be considered; if CD31, factor VIII, ERG, CD105, CD141, etc., are also positive, vascular endothelial tumors should be considered;
-
If desmin is positive, and Myogenin, MyoD1 are positive, rhabdomyosarcoma should be considered; if SMA, calponin, h-caldesmon are positive, smooth muscle tumors and myofibroblastic tumors should be considered;
-
If CD99 is positive, and NKX2.2 is positive, PNET/Ewing sarcoma should be considered; if STAT6 is positive, solitary fibrous tumor should be considered;
-
If S100 is positive, neuroectodermal tumors, neurogenic tumors, nerve sheath tumors, neuroblastoma, chondrogenic tumors, and lipogenic tumors should be considered; if actin, HMB45, and Melan A are positive, PEComa should be considered; if HMB45, Melan A, tyrosinase, SOX-10 are positive, malignant melanoma should be considered;
-
If osteonectin, osteopontin, SATB-2 are positive, bone tumors or osteosarcoma should be considered;
-
If LCA is positive, please refer to the immunohistochemical protocols for lymphoma.
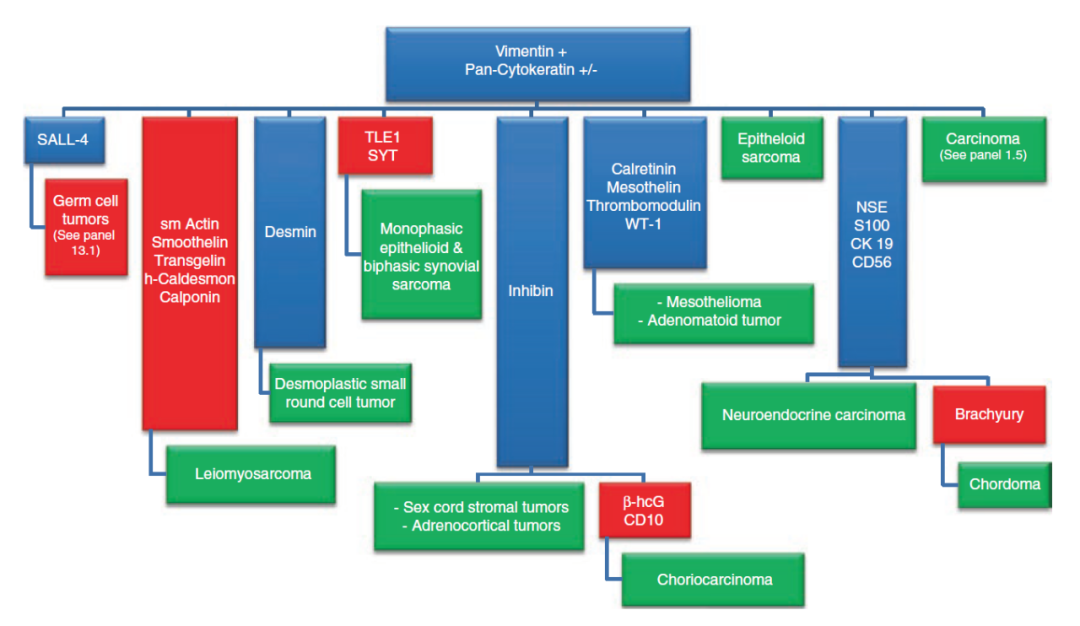
Figure 3. Immunohistochemical diagnostic approach for tumors positive for Vimentin and positive or negative for broad-spectrum CK.
Detailed Explanation of Figure 3
-
If SALL-4 is positive, germ cell tumors should be considered;
-
If SMA, smoothelin, transgelin, h-Caldesmon, Calponin are positive, leiomyosarcoma should be considered;
-
If desmin is positive, desmoplastic small round cell tumor should be considered;
-
If TLE1 is positive or there is SYT gene fusion, monophasic epithelioid synovial sarcoma and biphasic synovial sarcoma should be considered;
-
If inhibin is positive, sex cord-stromal tumors, adrenal cortical tumors should be considered; if inhibin is positive and β-hCG and CD10 are also positive, choriocarcinoma should be considered;
-
If calretinin, mesothelin, thrombomodulin, WT-1 are positive, mesothelioma, adenomatoid tumor should be considered;
-
If NST, S100, CK19, CD56 are positive, neuroendocrine carcinoma should be considered; if brachyury is added and positive, chordoma should be considered.
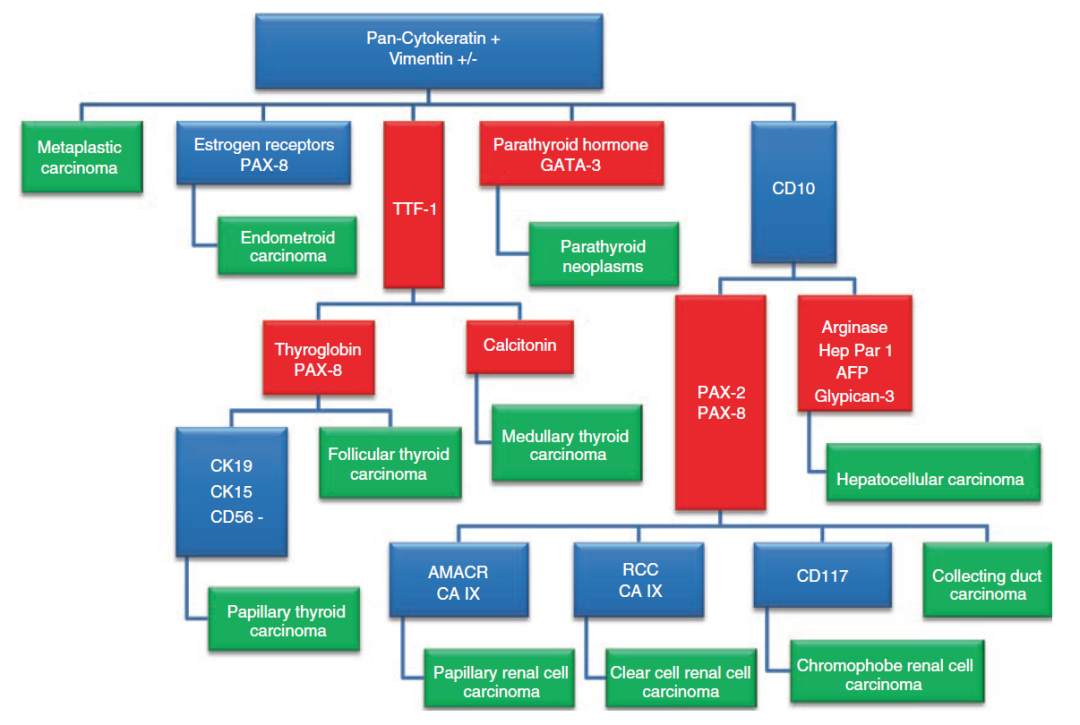
Figure 4. Immunohistochemical diagnostic approach for tumors positive for broad-spectrum CK and positive or negative for Vimentin.
Detailed Explanation of Figure 4
-
If ER, PAX-8 are positive, endometrioid carcinoma should be considered;
-
If TTF-1, Tg, PAX-8 are positive, tumors of thyroid follicular epithelial origin should be considered, such as thyroid follicular carcinoma; if CK19 is positive, CD15 is positive, and CD56 is negative, it supports papillary thyroid carcinoma; if TTF-1, CT are positive, medullary thyroid carcinoma should be considered;
-
If parathyroid hormone and GATA-3 are positive, it supports parathyroid tumors;
-
If CD10, arginase, Hep Par1, AFP, Glypican-3, etc., are positive, hepatocellular carcinoma should be considered;
-
If CD10, PAX-2, PAX-8 are positive, renal carcinoma should be considered, and further subtyping can be done based on other data: A, if AMACR, CA IX are positive, papillary renal cell carcinoma should be considered; B, if RCC, CA IX are positive, clear cell renal cell carcinoma should be considered; C, if CD117 is positive, chromophobe renal cell carcinoma should be considered; D, based on morphology and other findings, collecting duct carcinoma can also be considered.
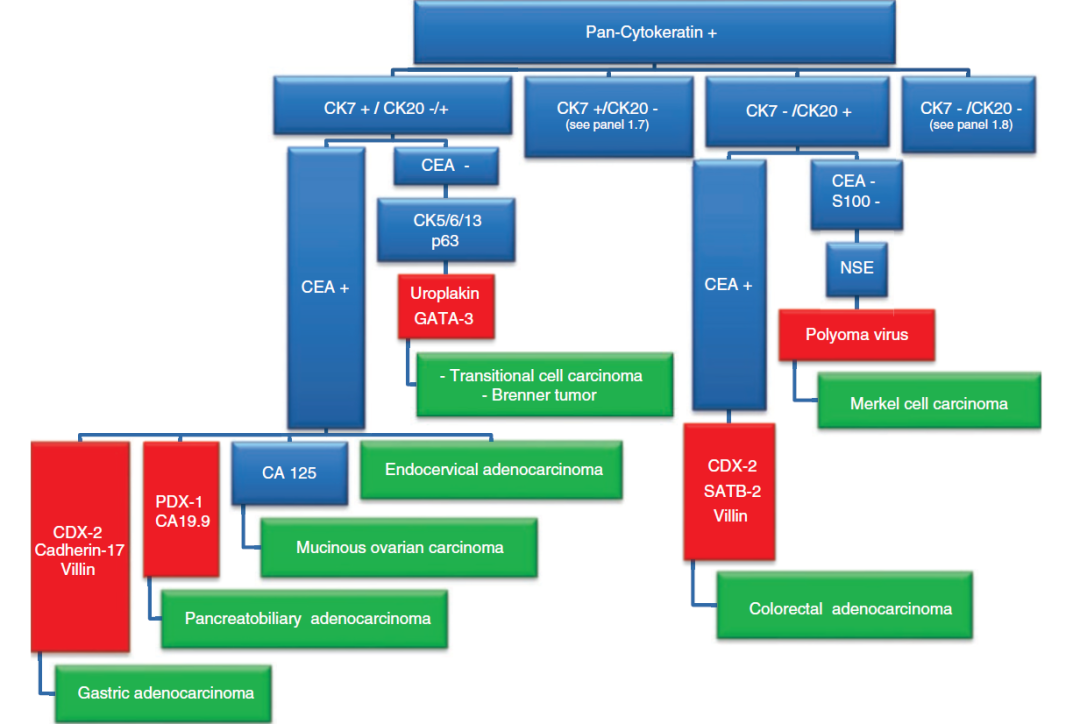
Figure 5. Immunohistochemical diagnostic approach based on CK7 and CK20 results in carcinoma.
Detailed Explanation of Figure 5
1. For CK7 positive/CK20 negative, CK7 negative/CK20 negative cases, a dedicated chart will be detailed later;
2. If CK7 is positive and CK20 is negative or positive, further analysis should be based on CEA status: A, if CEA is negative, and CK5/6, CK13, p63 are positive and Uroplakin, GATA-3 are positive, consider transitional cell carcinoma, Brenner tumor; B, if CEA is positive, cervical adenocarcinoma can be considered. Further analysis can also be done based on CEA positivity combined with other data: C, if CDX-2, Cadherin-17, Villin are positive, gastric adenocarcinoma should be considered; D, if PDX-1, CA19-9 are positive, pancreatobiliary adenocarcinoma should be considered; E, if CA125 is positive, ovarian mucinous carcinoma should be considered;
3. If CK7 is negative and CK20 is positive, further analysis can also be based on CEA status: A, if CEA is positive, and CDX-2, SATB-2, Villin are positive, colorectal adenocarcinoma should be considered; B, if CEA is negative, S100 is negative, and NSE, polyoma virus are positive, Merkel cell carcinoma should be considered.
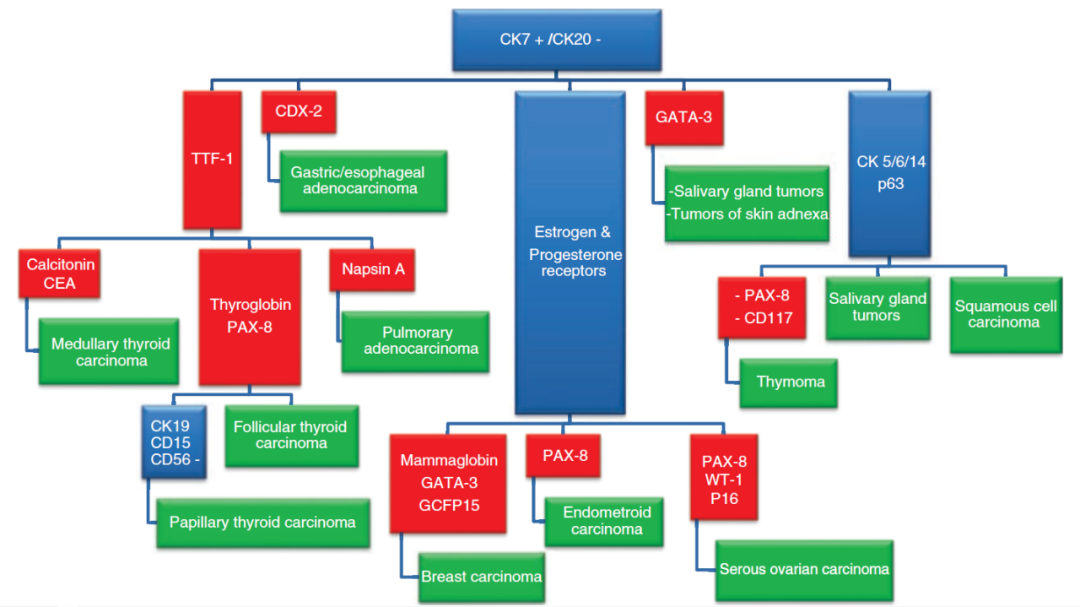
Figure 6. Immunohistochemical diagnostic approach for CK7 positive, CK20 negative carcinoma.
Detailed Explanation of Figure 6
-
If TTF-1 is positive, further subtyping can be done based on other data:A, if CT, CEA are positive, consider medullary thyroid carcinoma;B, if Tg, PAX-8 are positive, consider carcinoma of thyroid follicular epithelial origin;If CK19 is positive, CD15 is positive, and CD56 is negative, consider papillary thyroid carcinoma;C, if Napsin A is positive, consider lung adenocarcinoma;
-
If ER, PR are positive, further subtyping can be done based on other data: A, if mammaglobin, GATA-3, GCDFP-15 are positive, consider breast cancer; B, if PAX-8 is positive, consider endometrioid carcinoma; if PAX-8, WT-1, p16 are positive, consider ovarian serous carcinoma;
-
If only GATA-3 is positive, salivary gland tumors, skin adnexal tumors can be considered;
-
If CK5/6, CK14, p63 are positive, salivary gland tumors, squamous cell carcinoma can be considered; if PAX-8, CD117 are also positive, consider thymic tumors.
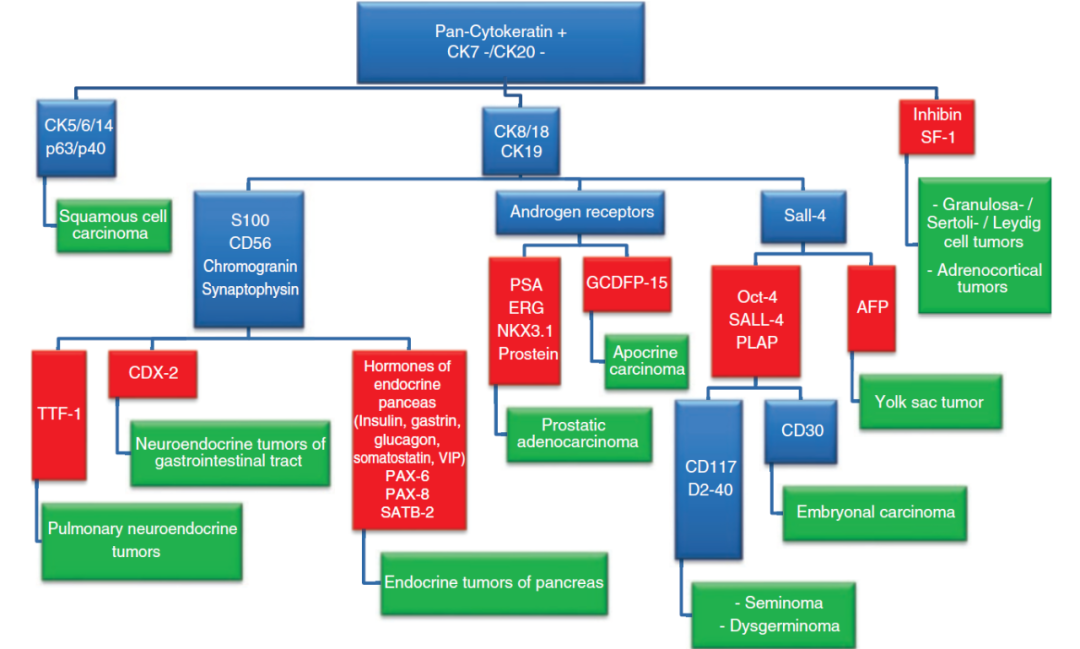
Figure 7. Immunohistochemical diagnostic approach for broad-spectrum CK positive but CK7 negative, CK20 negative carcinoma.
Detailed Explanation of Figure 7
-
If CK5/6, CK14, p63, p40 are positive, consider squamous cell carcinoma;If inhibin, SF-1 are positive, consider adrenal cortical tumors or ovarian granulosa cell tumor, Sertoli-Leydig cell tumor;
-
If CK8/18, CK19 are positive and S100, CD56, CgA, Syn are positive, further subtyping can be done based on other data: A, if TTF-1 is positive, consider pulmonary neuroendocrine tumor; B, if CDX-2 is positive, consider gastrointestinal neuroendocrine tumor; C, if pancreatic-related hormones (insulin, gastrin, glucagon, somatostatin, vasoactive intestinal peptide), PAX-6, PAX-8, SATB-2 are positive, consider pancreatic neuroendocrine tumor;
-
If CK8/18, CK19 are positive and AR is positive, further subtyping can be done based on other data: A, if PSA, ERG, NKX3.1, prostein are positive, consider prostate adenocarcinoma; B, if GCDFP-15 is positive, consider apocrine carcinoma;
-
If CK8/18, CK19 are positive and SALL-4 is positive, further subtyping can be done based on other data: A, if Oct-4, PLAP are positive, and CD30 is positive, consider embryonal carcinoma; if CD117, D2-40 are positive, consider seminoma, dysgerminoma; B, if AFP is positive, consider yolk sac tumor.