
Thirteenth Issue of “Mai Mai” Pathology Weekly Reading Notes | Immunohistochemical Markers for Hepatobiliary Tumors
Preface:
The anatomical positions and even histogenesis of the liver and gallbladder are closely related; in practical work, liver and gallbladder-related lesions often require comprehensive consideration, such as the differentiation between intrahepatic cholangiocarcinoma and hepatocellular carcinoma. Immunohistochemistry plays an important role in this. This section provides a detailed introduction to the immunohistochemical markers for common liver and gallbladder tumors, hoping to assist pathology colleagues in daily diagnosis.

The immunohistochemical marker status of common liver and gallbladder tumors is detailed in Table 1.
Table 1. Overview of Commonly Used Immunohistochemical Markers for Hepatobiliary Tumors
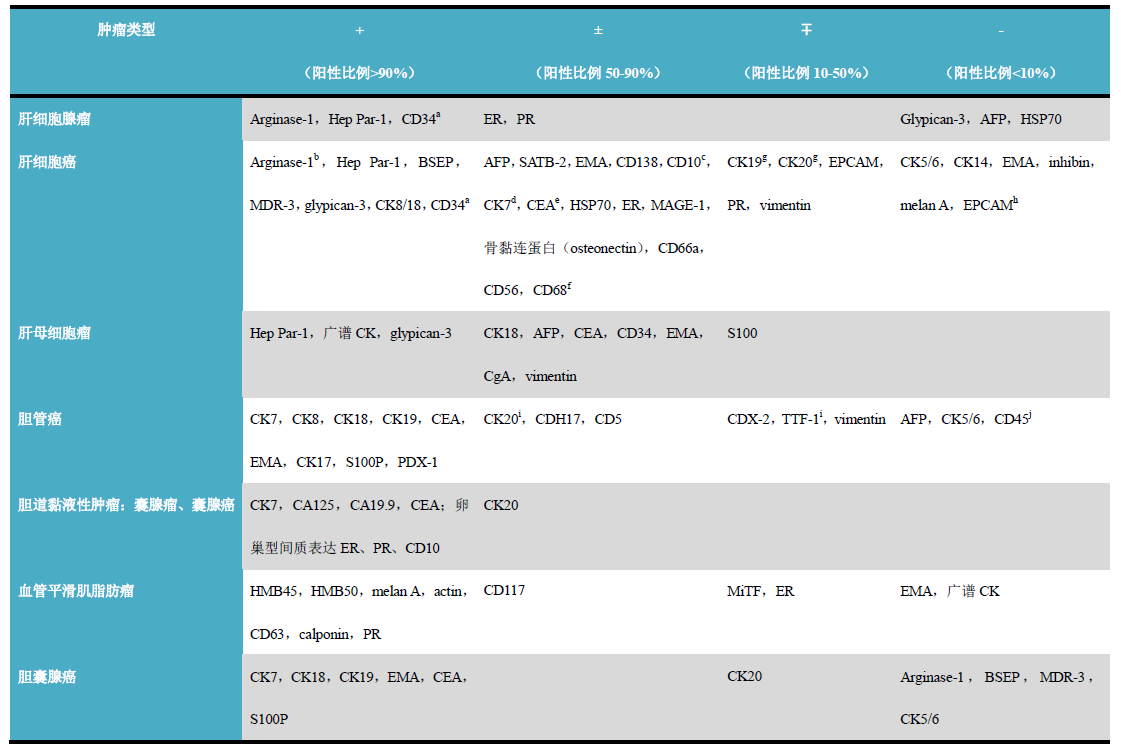
(Click to view larger image)
Remarks
-
Marks the sinusoidal endothelial cells within the tumor trabeculae; normal liver parenchyma does not express or rarely expresses it.
-
The degree of positive expression is related to the differentiation of hepatocellular carcinoma;
-
Apical staining of small bile ducts;
-
Strongly positive staining in fibrolamellar hepatocellular carcinoma, up to 50% staining in classical hepatocellular carcinoma, but normal hepatocytes are generally negative;
-
Only polyclonal CEA shows small bile duct staining, while monoclonal antibodies are negative;
-
Positive in fibrolamellar hepatocellular carcinoma, negative in classical hepatocellular carcinoma and normal hepatocytes;
-
Normal hepatocytes are negative;
-
EPCAM (BerEP-4) is generally positive in hepatoid carcinoma but negative in hepatocellular carcinoma;
-
CK20 and TTF-1 positivity are unique features of carcinomas originating from extrahepatic bile ducts; intrahepatic bile duct carcinomas are generally negative;
-
CD56 positivity is seen only in a very small number of carcinomas originating from intrahepatic bile ducts.
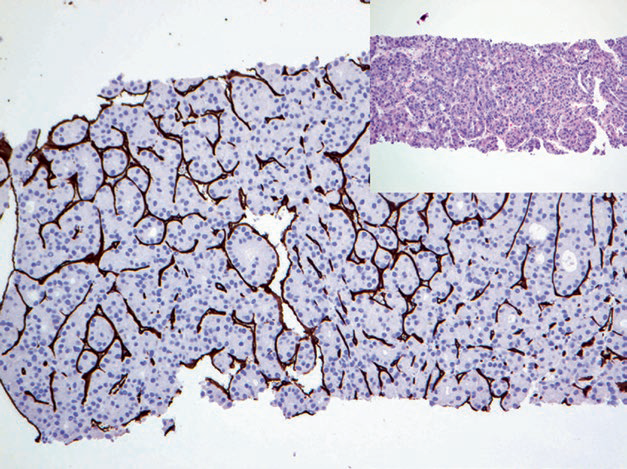
Figure 1. Hepatocellular carcinoma, immunohistochemistry CD34, sinusoidal endothelial cells positive.
Detailed Explanation of Some Immunohistochemical Indicators for Hepatocellular Tumors
Hepatocyte
Positive expression pattern: Cytoplasmic (granular staining)
Recommended positive control tissue: Liver tissue
Arginase-1
Alpha-fetoprotein
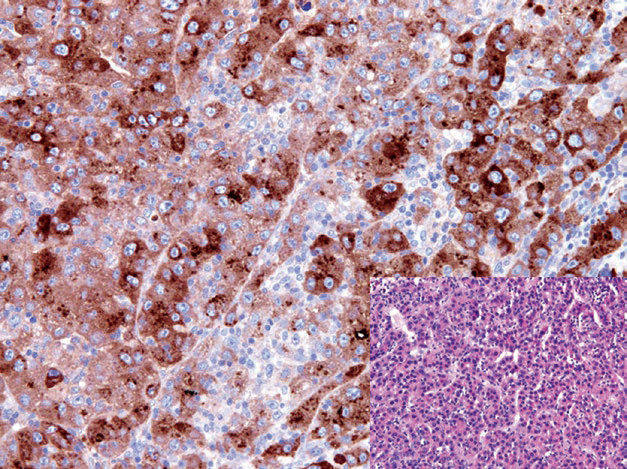
Figure 2. Hepatocellular carcinoma, tumor cells strongly positive for AFP.
Positive expression pattern: Cytoplasmic
Recommended positive control tissue: Fetal liver tissue
Glypican-3
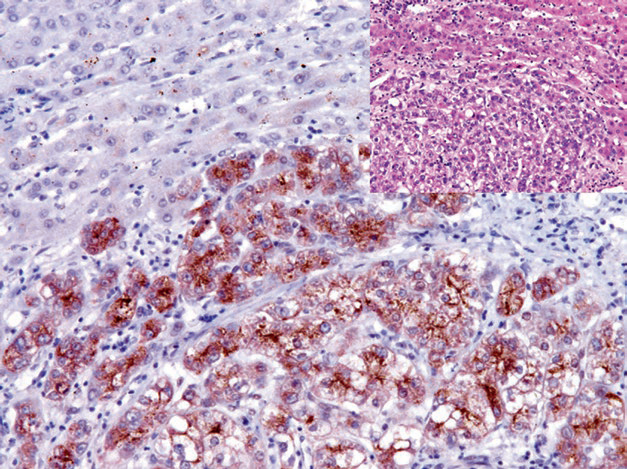
Figure 3. Hepatocellular carcinoma, immunohistochemistry Glypican-3 positive; non-neoplastic liver tissue in the background is negative.
BSEP and MDR-3
HSP70
1
Mai Mai: “Arginase-1 is a sensitive and specific marker for hepatocellular adenoma and hepatocellular carcinoma, and can be combined with Glypican-3 and Hepatocyte for the differential diagnosis of primary hepatocellular carcinoma from metastatic tumors and cholangiocarcinoma.。Glypican-3 is expressed in embryonic liver, kidney, lung tissues, and the trophoblast layer of placental tissue, while other normal tissues do not express it,Positive expression can be seen in neoplastic tissues such as hepatocellular carcinoma, yolk sac tumor, choriocarcinoma, and melanoma. Combined use with CD34 can help differentiate benign from malignant hepatocellular tumors.”
|
Antibody Name |
Clone Number |
Positive Control |
Positive Location |
|
Arginase-1 |
EP261 |
Liver, Liver Cancer |
Cytoplasmic/Nuclear |
|
Hepatocyte |
OCH1E5 |
Liver Tissue, Hepatocellular Carcinoma |
Cytoplasmic |
|
Glypican-3* |
MAXIM001 |
Liver Cancer, Placenta |
Cytoplasmic |
*Marked as Maxin Clone Products
For more information, please contact: 800-8581156 or 400-889-9853