
Pathology Weekly Reading Notes by “Mai Mai” | Issue 1
Preface:
In the world of pathology, one phrase that pathologists frequently encounter is, ‘Let’s do immunohistochemistry…’
Indeed, if pathology were a martial arts world, routine diagnosis would be akin to basic hand-to-hand combat, while immunohistochemistry would be the weapon or hidden weapon: to some extent, it is more powerful and precise in pathological diagnosis.
However, precisely because pathology is a martial arts world, the choice of weapon or hidden weapon is extremely nuanced: just considering swords, should one use the ‘heavy sword without an edge, great skill appears clumsy’ Xuantie heavy sword, or the uniquely shaped and oddly used Golden Snake Sword? This depends on the ‘enemy’ faced (specific disease types and differential diagnoses), while also considering one’s own conditions (such as laboratory capabilities). After all, it’s hard to imagine the majestic Fourth Master of the Red Flower Society, Wen Tailai, spitting date pit nails!
Recently, the editor had the privilege of reading Springer’s book ‘Immunohistochemistry in Tumor Diagnostics.’ The book provides detailed insights into the key applications of immunohistochemistry in tumor diagnosis, including recommended ‘panels’ for different diseases and explanations of specific marker applications. We have compiled our reading notes to share with everyone, hoping to provide as much assistance as possible in your work.
Overview of Immunohistochemistry
Staining Patterns of Immunohistochemical Markers
-
Nuclear Staining: This occurs when antigens are expressed in the nucleus or nuclear membrane; examples include transcription factors and steroid hormone receptors.
-
Cytoplasmic Staining: This occurs when antigens are localized in the cytoplasm; examples include cytoskeletal proteins (vimentin, actin, desmin, CK). Some antigens can be further subdivided within the cytoplasm, such as localization to mitochondria (resulting in granular cytoplasmic staining) or the Golgi apparatus (resulting in perinuclear staining).
-
Membrane Staining: This occurs when antigens are localized on the cell membrane; typical examples include most CD series antigens.
-
Extracellular Staining: This involves staining of extracellular and tissue matrix antigens, as well as secreted products of cells; examples include collagen components and CEA.
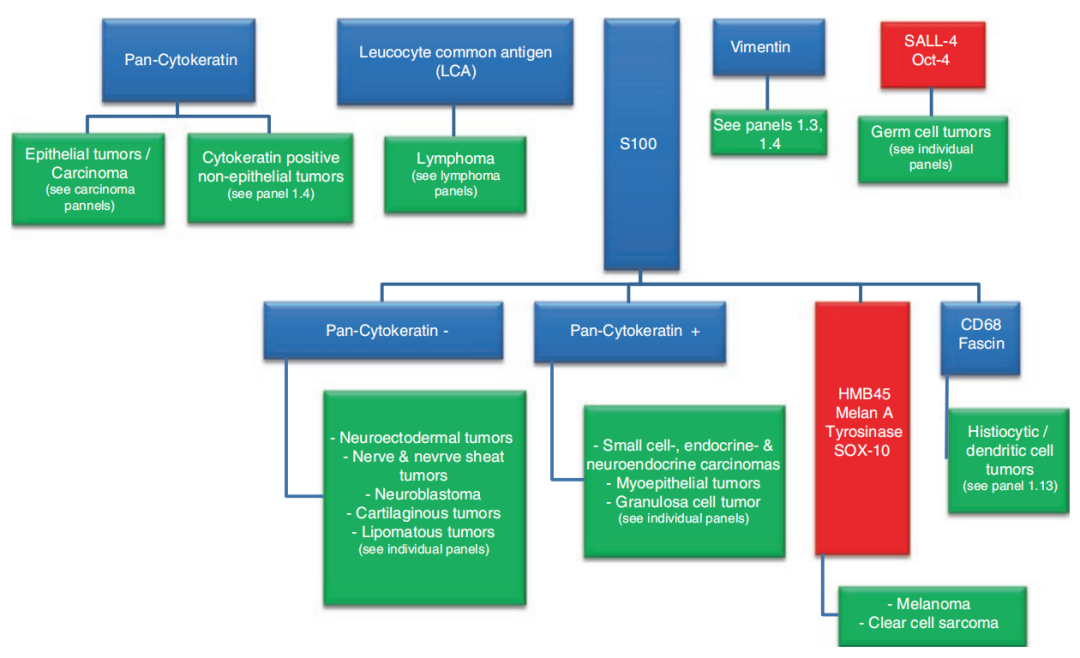
Immunohistochemistry ‘Panels’ in Tumor Diagnosis
-
If broad-spectrum CK is positive, there are two considerations: epithelial tumors (malignant cases are carcinomas) and CK-positive non-epithelial tumors.
-
If LCA is positive, lymphoma is often considered; details will be discussed later.
-
If vimentin is positive, the situation is more complex and requires detailed analysis combined with CK status; details will be discussed later.
-
If SALL-4 or Oct-4 is positive, germ cell tumors are often considered.
-
If S100 is positive, further analysis with other markers is needed: A. If broad-spectrum CK is negative, consider neuroectodermal tumors, neurogenic tumors, nerve sheath tumors, neuroblastoma, chondroid tumors, lipomatous tumors, etc.; B. If broad-spectrum CK is positive, consider small cell carcinoma, neuroendocrine carcinoma, myoepithelial tumors, granular cell tumors, etc.; C. If HMB45, Melan A, tyrosinase, or SOX-10 are positive, consider malignant melanoma, clear cell sarcoma; D. If CD68 or Fascin is positive, consider histiocytic/dendritic cell tumors.
To be continued…….