Somatostatin (SST) is a regulatory peptide widely present in various organs of the human body, acting on endocrine, exocrine, paracrine, and autocrine functions. It exerts inhibitory effects on cell proliferation, angiogenesis, and induction of apoptosis. The biological activity of somatostatin is mediated by G protein-coupled somatostatin receptors (SSTR) on target cell membranes.
There are five subtypes of SSTRs, which are widely expressed in normal tissues and neuroendocrine tumors, exhibiting subtype selectivity and tissue specificity. SSTR1-3 are expressed in both tumor cells and non-tumor epithelial cells, while SSTR4 is expressed only in epithelial cells.For example, in functional pituitary adenoma tissues, growth hormone-secreting adenomas mainly express SSTR2 and SSTR5, while prolactinomas express SSTR1, SSTR2, and SSTR5, with very low expression of SSTR4. Most neuroendocrine tumors and their metastases express SSTR2 at higher levels than normal tissues. Primary liver tumors and medullary thyroid carcinoma also show high expression of SSTR2. Functionally, both SSTR3 and SSTR2 can mediate the release of somatostatin, thereby inhibiting endothelial cell proliferation and inducing apoptosis. SSTR2 is involved in the body’s anti-tumor response, and its low expression may promote tumor cell proliferation and migration.
SSTR2 as a Prognostic Indicator for Neuroendocrine Tumors
Neuroendocrine tumors are relatively rare, accounting for less than 1% of all malignant tumors, and often occur in the stomach, intestines, and pancreas. According to the 2019 WHO Fifth Edition Classification of Digestive System Tumors, neuroendocrine tumors are divided into well-differentiated and poorly differentiated based on their degree of differentiation. The former are neuroendocrine tumors (NETs), while the latter are neuroendocrine carcinomas (NECs). NECs have a worse prognosis and do not benefit from treatment with somatostatin and its analogs. Multiple studies have shown that well-differentiated tumor cells typically have high SSTR expression, while poorly differentiated tumor cells have low SSTR expression.
Liu Zhongyuan et al. performed SSTR2 immunohistochemical detection on 56 patients with colorectal neuroendocrine tumors and found a positive expression rate of SSTR2 of 76.8% (43/56). Positive expression of SSTR2 was closely related to lymph node metastasis, tumor invasion of the muscular layer, and distant metastasis (P < 0.05). As the histological grade of colorectal neuroendocrine tumors decreased, the maximum tumor diameter increased, muscular layer invasion occurred, lymph node metastasis occurred, and distant metastasis occurred, the malignant degree of the tumor increased, and the low expression of SSTR2 protein became more pronounced. Therefore, SSTR2 detection may serve as one of the prognostic indicators for colorectal neuroendocrine tumors.
Yang Xiaodong’s study also yielded similar results: among 121 colorectal specimens, 58 cases showed low SSTR2 expression, and 63 cases showed high expression. Among the 111 patients who were followed up, the 5-year overall survival rate was 70%, with the low SSTR2 expression group (53%) significantly lower than the high expression group (83%). Analysis confirmed that SSTR2 expression level can serve as an independent prognostic indicator.
In two research institutions in Italy and Japan, SSTR2 immunohistochemical staining (using automated and manual methods) was performed on 52 tissues from 38 neuroendocrine tumor patients. Three professional pathologists and medical students independently evaluated the stained sections using three different scoring systems (Volante score, Her2 score, and H score). The evaluation results showed very high consistency regardless of the staining method or the evaluator’s experience. Among them, the HER2 and H scores reliably represented patient characteristics, and SSTR2 expression assessed by the HER2 score was significantly correlated with the clinical efficacy of somatostatin analogs (P=0.04).
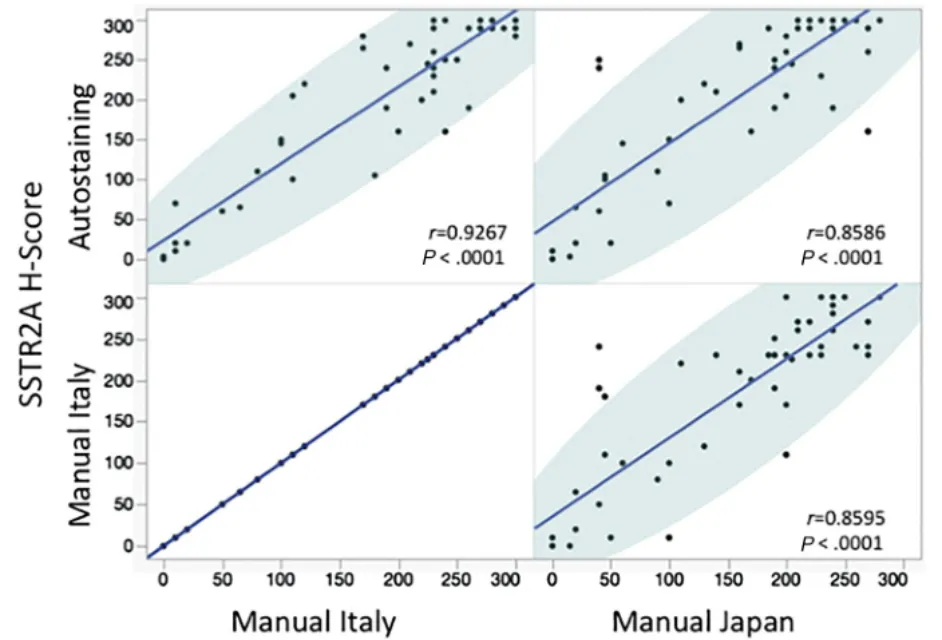
Figure 1: Scatter plot analysis with linear regression and 95% confidence intervals for SSTR2 detection results using three different staining methods
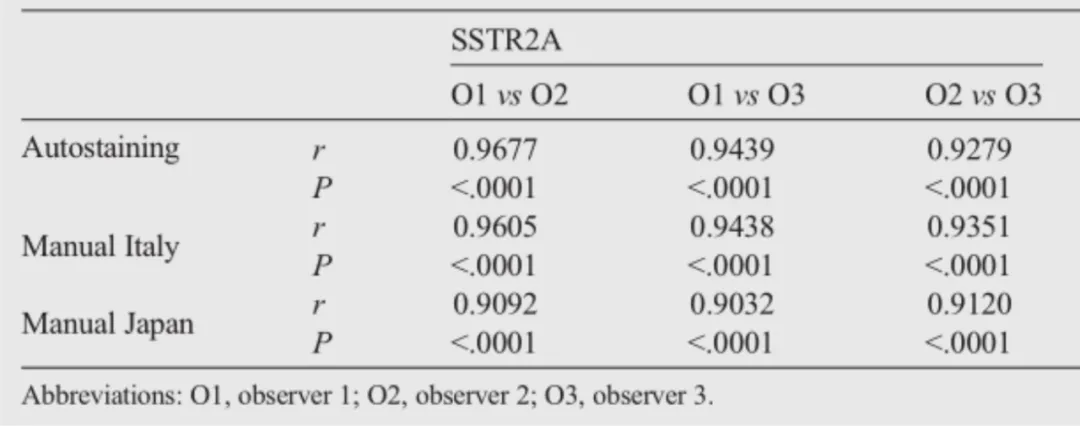
Table 1: Consistency among three evaluators in assessing SSTR2 detection results using three staining methods
The ‘Chinese Expert Consensus on Gastrointestinal and Pancreatic Neuroendocrine Tumors (2020 Edition)’ states that when diagnosing neuroendocrine tumors, somatostatin markers can be used to guide the clinical use of somatostatin analogs for treatment. Clinically, somatostatin receptor scintigraphy (SRS) and PET-CT techniques are often used for detection. Studies have found that the intensity of SSTR2 expression is positively correlated with somatostatin receptor functional imaging findings and also has prognostic significance. Using immunohistochemistry to detect SSTR2 levels is simpler and easier to standardize. The guidelines recommend scoring SSTR2 staining results with reference to the gastric cancer HER2 interpretation criteria: 0 points: no staining; 1+: weak cell membrane staining in at least 10% of tumor cells; 2+: weak to moderate intensity cell membrane staining in at least 10% of tumor cells; 3+: strong cell membrane staining in at least 10% of tumor cells.
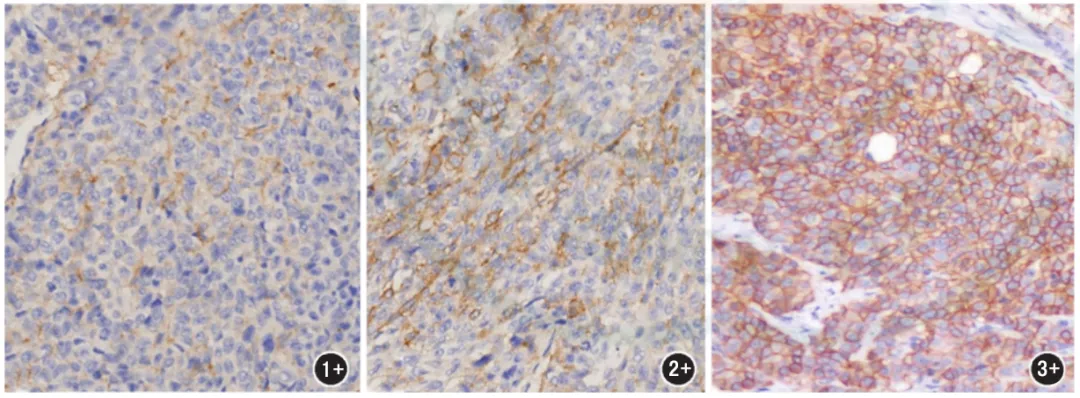
Figure 2: SSTR2 protein expression levels in neuroendocrine tumors (1+,2+,3+)
Therefore, when using immunohistochemistry to detect SSTR2 expression levels, finding a reliable and high-performance SSTR2 antibody is key for clinical application. Maixin SSTR2 uses a rabbit monoclonal antibody with high sensitivity, good stability, minimal antigen cross-reactivity, higher potency than other polyclonal antibodies, and superior staining.
Maixin Related Antibodies
|
Antibody Name
|
Product Number
|
Clone Number
|
Positive Location
|
|
SSTR2
|
RMA-0860
|
EP149
|
Cytoplasm/Cell Membrane
|
References:
[1]Kasajima A, Papotti M, Ito W, et al. High interlaboratory and interobserver agreement of so-matostatin receptor immunohistochemical determi-nation and correlation with response to somato-statin analogs. Hum Pathol. 2018 Feb;72:144-152.
[2] Liu Zhongyuan, Zhang Chong, Zhang Li. Expression and significance of somatostatin receptor 2 in colorectal neuroendocrine tumors [J]. World Chinese Journal of Digestology, 2016, 24(18): 2817-2822.
[3] Yang Xiaodong, Huang Ping, Wang Feng, et al. Relationship between expression of somatostatin receptor 2 and prognosis in colorectal cancer [J]. Chinese Journal of Gastrointestinal Surgery, 2010, 13(12): 940-941. DOI: 10.3760/cma.j.issn.1671-0274.2010.12.019
[4] Chinese Consensus on Pathological Diagnosis of Gastrointestinal and Pancreatic Neuroendocrine Tumors (2020 Edition). Chinese Journal of Pathology, January 2021, Vol. 50, No. 1
