Overview of immunohistochemistry for the diagnosis of thyroid and parathyroid tumors
For immunohistochemistry of thyroid tumors, the selection of specific markers should first be considered based on the cell of origin. Tumors derived from follicular epithelial cells can choose: Tg, TPO, TTF-1, PAX-8, galectin-3, HBME-1, CD56, Trop-2, CK19, and other CKs; tumors derived from C cells should consider CT, TTF-1, CEA, and other neuroendocrine markers.
Table 1. Overview of immunohistochemistry for thyroid tumor diagnosis
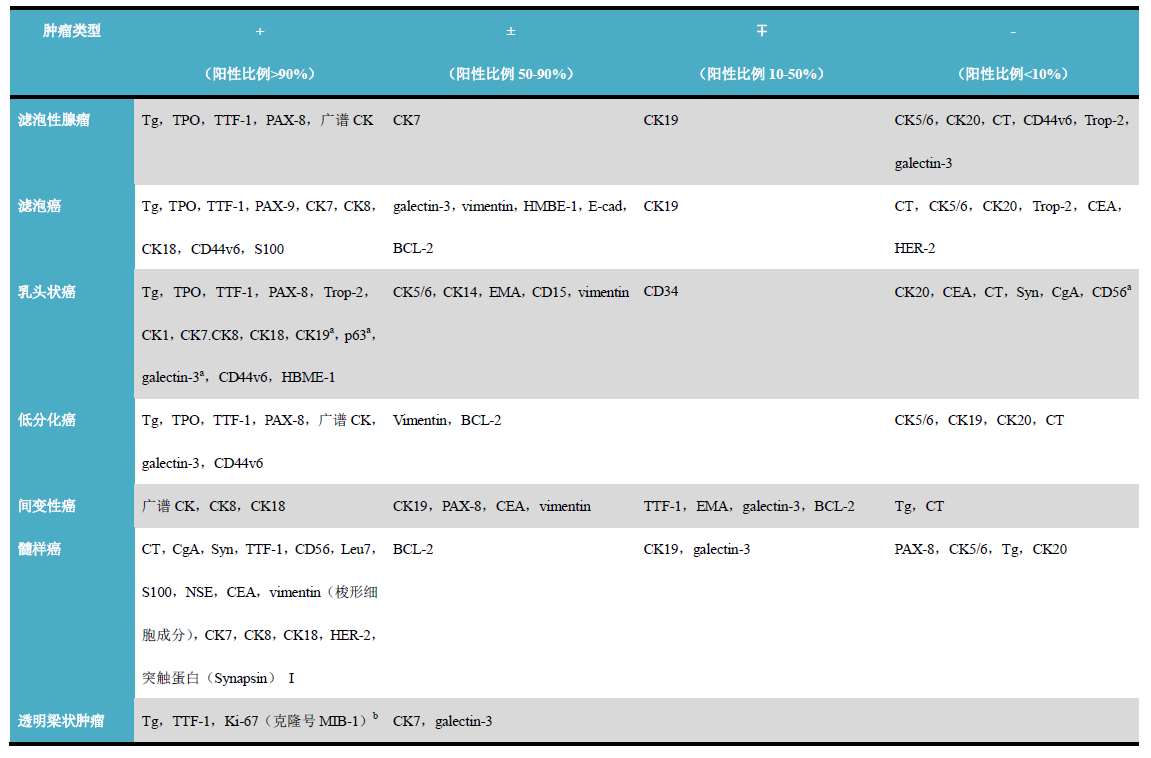
(Click to view larger image)
Notes
-
Expression differences mainly lie in the immunohistochemical differentiation between papillary thyroid carcinoma, benign papillary hyperplasia, and follicular tumors; specifically, CK19 is positive in papillary thyroid carcinoma, negative or weakly positive in follicular tumors, but may be positive in lymphocytic thyroiditis; galectin-3 is positive in papillary carcinoma and follicular carcinoma, negative in benign thyroid tissue; CD56 is negative in papillary thyroid carcinoma, positive in benign thyroid tissue, papillary hyperplasia, and follicular tumors; p63 is focally positive in papillary carcinoma, negative in other lesions except papillary thyroid carcinoma; Trop-2 is positive in over 90% of papillary thyroid carcinomas, negative in follicular adenoma and follicular carcinoma.
-
When detected using the MIB-1 clone, staining patterns may appear on the cell membrane and cytoplasm, which is a characteristic immunohistochemical staining manifestation of this tumor.
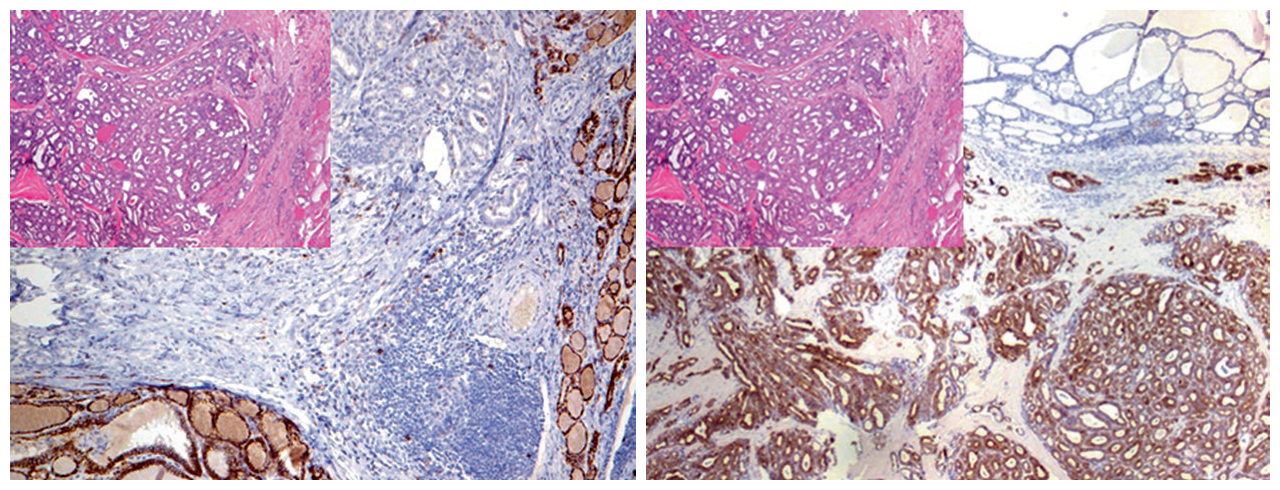
Figure 1. (Left) Normal thyroid tissue is CD56 positive, while papillary thyroid carcinoma does not express it. (Right) Papillary thyroid carcinoma is CK19 positive, while normal thyroid tissue does not express it.
Commonly used immunohistochemical markers for parathyroid tumor diagnosis include PTH, Tg, TTF-1, PAX-8.
Table 2. Overview of immunohistochemistry for parathyroid tumor diagnosis
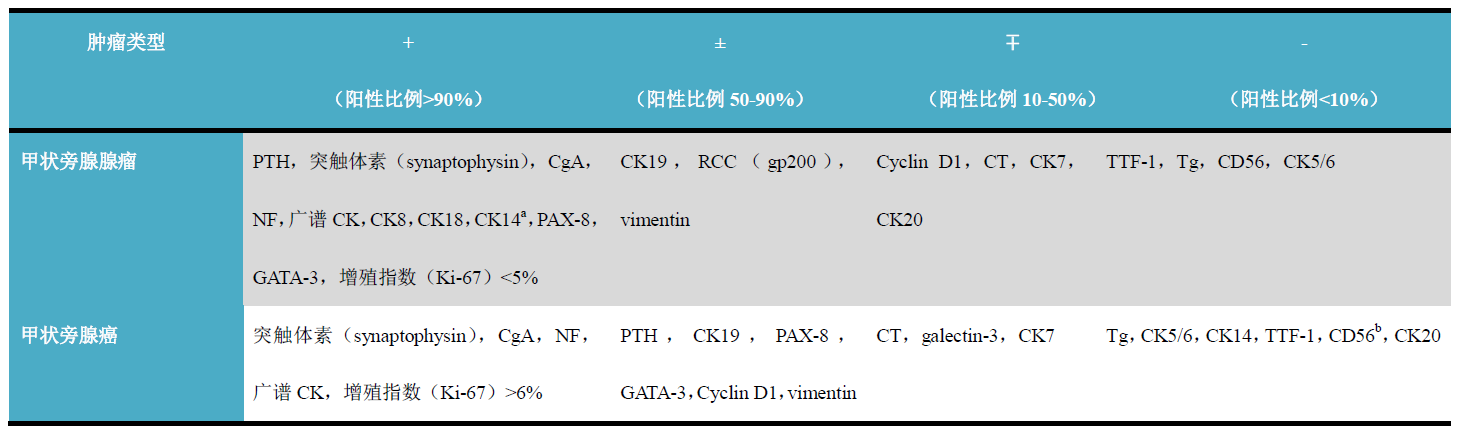
(Click to view larger image)
Notes
-
Negative in parathyroid carcinoma;
-
May be positive in oxyphilic parathyroid adenoma.
Detailed explanation of some markers
Positive expression pattern: Cytoplasm
Recommended positive control tissue: Thyroid tissue
Tg is a glycoprotein synthesized by thyroid follicular cells and is the raw material for thyroid hormone synthesis; therefore, Tg is a specific marker for thyroid follicular cells and tumors derived from follicular cells. Except for C cells and related tumors, which do not express this marker, thyroid anaplastic carcinoma generally also does not express Tg. In practical work, it is recommended to use Tg in combination with TTF-1 and Pax-8 to differentiate between lung cancer and thyroid cancer.
For thyroid follicular cells, TPO is relatively more specific; at the same time, the expression of this marker is related to the differentiation degree of tumors derived from thyroid follicular epithelium, and it can be negative in poorly differentiated thyroid carcinoma.
Positive expression pattern: Cytoplasm
Recommended positive control tissue: Appendix
In the lung chapter, TTF-1 has been discussed in detail. In addition to being expressed in lung cancer, TTF-1 can also be expressed in thyroid tissue and corresponding carcinomas: follicular carcinoma, papillary carcinoma, and medullary carcinoma can all show strong positive expression of TTF-1, but thyroid anaplastic carcinoma is generally negative.
TTF-2 is a nuclear protein involved in the synthesis of Tg and TPO, expressed in thyroid follicular cells, related tumors, a small number of C cells, anterior pituitary, esophageal and tracheal mucosa, and vas deferens. Lung parenchyma, gastrointestinal epithelium, hepatopancreatic epithelium, and tumors from these tissues generally do not express TTF-2.
Positive expression pattern: Cell membrane/cytoplasm
Recommended positive control tissue: Prostate tissue
Trophoblastic cell surface antigen 2 (Trop-2) is a transmembrane glycoprotein that functions as a calcium signal transducer. During malignant transformation, Trop-2 expression is upregulated. This marker is expressed in various types of carcinomas, such as gastrointestinal cancer, lung cancer, genitourinary tract cancer, and breast cancer. For thyroid tumors, over 90% of papillary thyroid carcinomas express Trop-2, while follicular adenoma and follicular carcinoma generally do not express it.
Positive expression pattern: Cell membrane
Recommended positive control tissue: Neuroblastoma
Pax-8 is a transcription factor related to the development of the fetal brain, eyes, thyroid tissue, upper urinary tract system, and Mullerian-derived organs. For thyroid tumors, over 90% of thyroid follicular carcinomas and papillary carcinomas, most poorly differentiated thyroid carcinomas, and over 50% of thyroid anaplastic carcinomas express this marker. Lung adenocarcinoma and breast cancer generally do not express Pax-8.
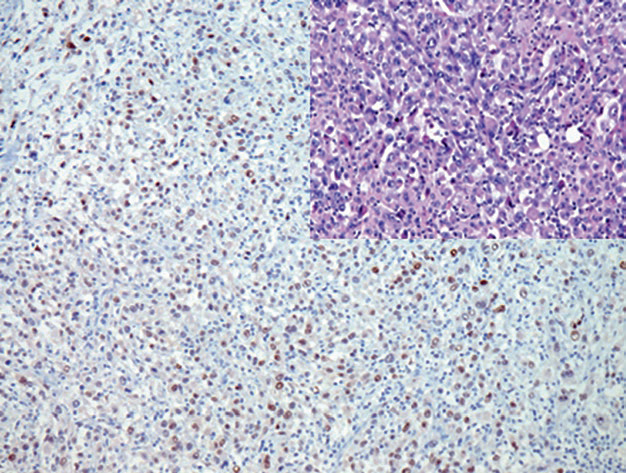
Figure 2. Thyroid anaplastic carcinoma, with nuclear expression of Pax-8.
Galectin-3 is a member of the galactoside-binding protein family. Its expression is activated during malignant transformation of tissues, so positivity for this marker aids in the diagnosis of various carcinomas: it is positive in most papillary thyroid carcinomas and follicular carcinomas, parathyroid carcinomas, head and neck squamous cell carcinomas, colorectal carcinomas, and hepatocellular carcinomas.
Pax-8 and GATA-3 are both positive in parathyroid glands and parathyroid tumors, such as adenomas and carcinomas, showing characteristic nuclear staining, so they can be used in combination with other parathyroid-related markers. Of course, it should be noted that thyroid follicular epithelium and related tumors also express Pax-8.
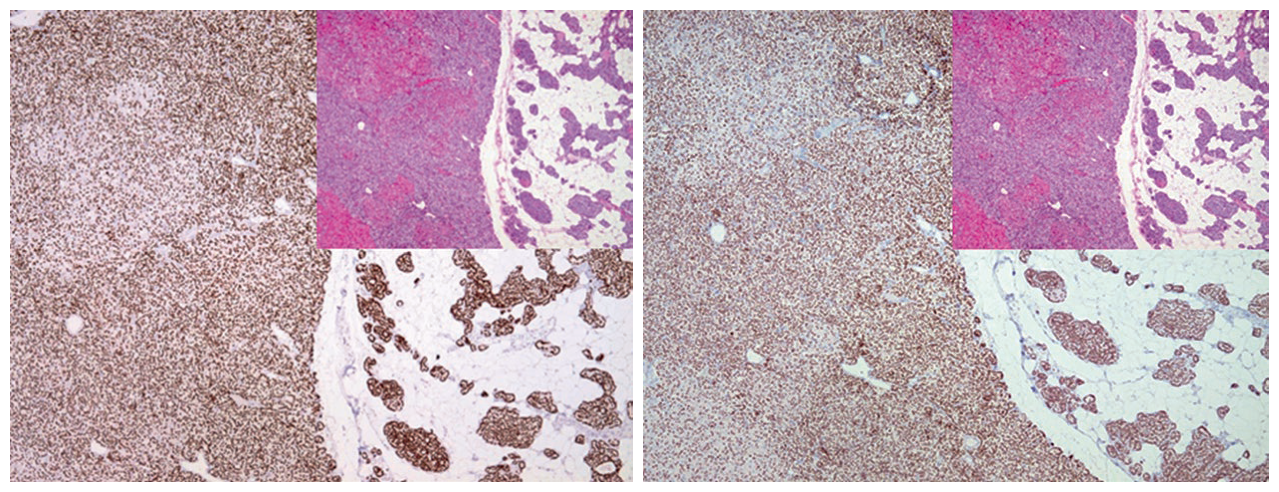
Figure 3. Parathyroid adenoma and compressed parathyroid tissue both express GATA-3 (left) and Pax-8 (right).
This is a surface glycoprotein expressed in various carcinomas, including papillary thyroid carcinoma. When used in combination with other markers, CD44v6 can be used to differentiate papillary thyroid carcinoma from other morphologically similar thyroid lesions.
Positive expression pattern: Cytoplasm
Recommended positive control tissue: Thyroid tissue/medullary carcinoma
Calcitonin (CT) is a polypeptide synthesized by C cells, therefore it is a specific marker for C cells and tumors derived from these cells (i.e., medullary carcinoma), while tumors derived from thyroid follicular epithelium do not express this marker but express TTF-1. It should be noted that some neuroendocrine tumors (such as pheochromocytoma) have been reported to express CT, but these tumors generally do not express TTF-1.
Positive expression pattern: Cytoplasm
Recommended positive control tissue: Parathyroid
Parathyroid hormone (PTH) is synthesized and secreted by the chief cells of the parathyroid glands. PTH and CT directly regulate the levels of calcium and phosphorus in the blood. Antibodies against PTH and related peptides are specific markers for the diagnosis of parathyroid tumors. PTH also helps in identifying ectopic parathyroid tissue and related tumors, which can occur in the mediastinum or thymus.

Figure 4. Both parathyroid adenoma and normal parathyroid tissue show positive expression of PTH.
It should be noted that although PTH is synthesized by the chief cells of the parathyroid glands, it is generally rapidly secreted, which may lead to false negatives in immunohistochemistry. Non-secretory clear cell type parathyroid carcinoma may resemble metastatic renal cell carcinoma or other clear cell carcinomas. In the diagnosis of thyroid and parathyroid tumors, immunohistochemistry should include thyroglobulin and parathyroid hormone markers based on other differential diagnostic markers.
Parathyroid hormone-related peptide
Parathyroid hormone-related peptide is a member of the parathyroid hormone family, also involved in calcium metabolism and regulating endochondral ossification. Antibodies against this hormone show positive expression in parathyroid cells and parathyroid tumors, and are also seen in some other malignant tumors, such as breast cancer, cholangiocarcinoma, transitional cell carcinoma, especially poorly differentiated carcinomas. This marker can also be used to differentiate cholangiocarcinoma from metastatic colorectal adenocarcinoma.
MaiXin Recommendation:”Good pathological diagnosis cannot be achieved without immunohistochemistry! And choosing high-quality, stable, and excellent-performing antibodies is half the success.”
|
Antibody Name
|
Clone Number
|
Positive Control
|
Cellular Localization
|
|
CD44V6*
|
MX072
|
Cervical cancer, Breast cancer
|
Membrane
|
|
CT
|
SP17
|
Thyroid tissue, Thyroid medullary carcinoma
|
Cytoplasm
|
|
Galectin-3*
|
MX060
|
Papillary thyroid carcinoma, Kidney |
Cytoplasm/Nucleus
|
|
Pax-8*
|
MX062
|
Renal clear cell carcinoma, Fallopian tube
|
Nucleus
|
|
PTH
|
MRQ-31
|
Parathyroid adenoma
|
Membrane/Cytoplasm
|
|
TTF-1*
|
MX011
|
Lung adenocarcinoma, Thyroid
|
Nucleus
|
*Marked as MaiXin clone products
For more information, please contact: 800-8581156 or 400-889-9853
