Overview of Immunohistochemistry for Pituitary Tumor Diagnosis
Regarding immunohistochemical testing in the diagnosis of pituitary tumors, it is first important to note that the pituitary can be divided into the adenohypophysis (i.e., anterior pituitary) and the neurohypophysis (i.e., posterior pituitary); the types of tumors that commonly occur in these two sites are significantly different, therefore, the selection of immunohistochemical markers also varies considerably.
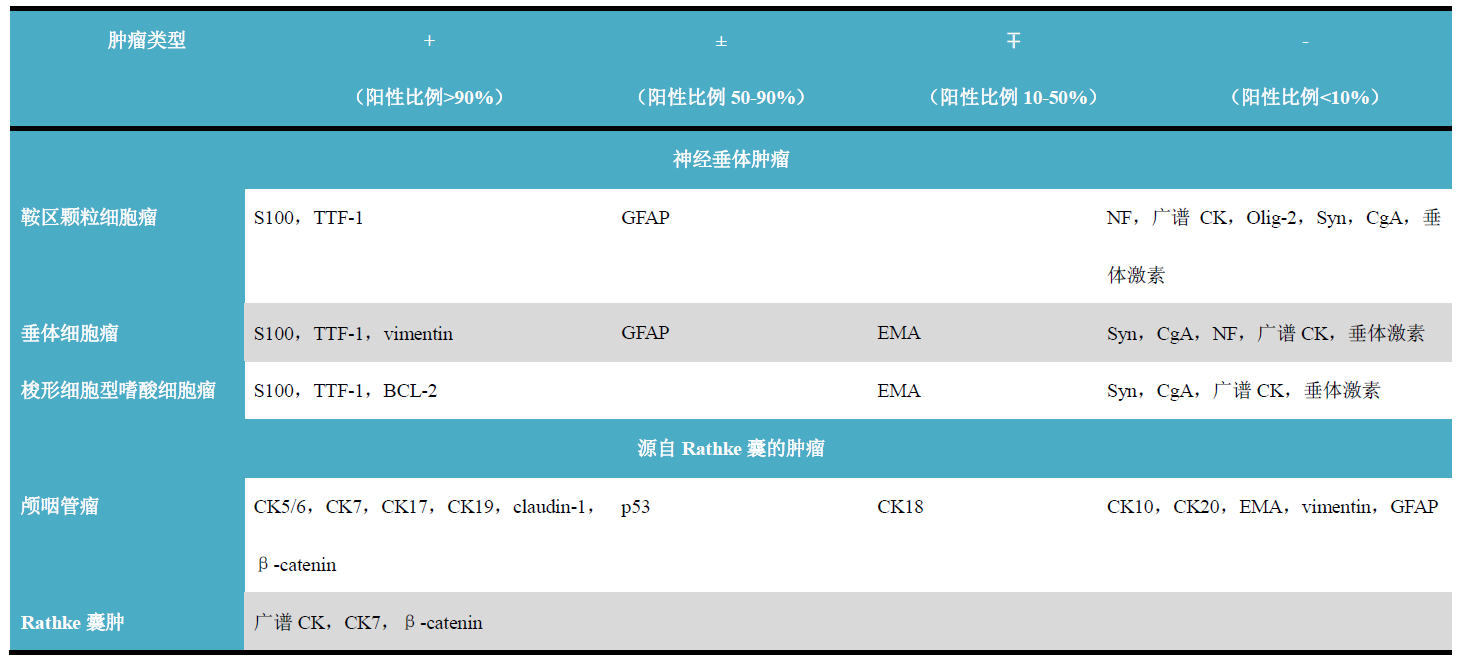
Table 1. Overview of Immunohistochemical Characteristics for Diagnosing Adenohypophyseal Tumors

(Click to view larger image)
Table 2. Overview of Immunohistochemical Characteristics for Neurohypophyseal Tumors and Other Tumors
(Click to view larger image)
For the adenohypophysis, commonly used immunohistochemical markers include the aforementioned neuroendocrine markers, certain CKs, and pituitary hormones; the first two are detailed in other chapters, this issue focuses on issues related to pituitary hormones. For the neurohypophysis, commonly used immunohistochemical markers include GFAP, S100, and TTF-1; the first two will be covered in chapters related to the central nervous system, this issue briefly introduces issues related to TTF-1.
Detailed Explanation of Pituitary Hormone Indicators
From a functional perspective, cells of the adenohypophysis can be divided into at least five types: α, β, δ, γ, ε. Different cells produce different hormones, and in most cases, one cell produces only one hormone. In fact, the current classification of pituitary adenomas is based on the hormonal activity of the related adenoma cells, which is also where immunohistochemistry using antibodies related to pituitary hormones and hormone precursor molecules comes into play.
-
Growth hormone (GH): Its function is to stimulate the release of insulin-like growth factor-1, which promotes long bone growth;
-
Prolactin (PRL): Antibodies against this hormone will label normal and neoplastic cells that produce prolactin; it should be noted that prolactin-producing cells can also be found in the prostate;
-
Thyroid-stimulating hormone (TSH): This hormone is composed of α and β subunits and regulates T4 production in the thyroid;
-
Adrenocorticotropic hormone (ACTH): The target of this hormone is adrenal cortical cells; however, besides being synthesized in the adenohypophysis, this hormone can also be synthesized by macrophages and lymphocytes under stress conditions. At the immunohistochemical level, small cell lung carcinoma can also express ACTH;
-
Follicle-stimulating hormone (FSH): This hormone is also composed of α and β chains, regulating folliculogenesis, spermatogenesis, and the proliferation of Sertoli cells;
-
Luteinizing hormone (LH): This hormone is composed of α and β chains, regulating folliculogenesis and the production of testosterone in Leydig cells;
-
α subunit (α-SU): Among pituitary hormones, all glycoprotein hormones are composed of the same α chain and somewhat different β chains. Expression of the α subunit can be seen in most adenomas producing TSH, FSH, and LH; however, some pituitary adenomas express only the α subunit.
-
TTF-1: This marker is detailed in lung tumors and the subsequently mentioned thyroid tumors. TTF-1 is also expressed in the neurohypophysis; therefore, this marker can serve as a label for tumors derived from related cells in the neurohypophysis, such as pituicytoma and granular cell tumor of the sellar region. These tumors do not express CK, which is a very crucial point in differential diagnosis.
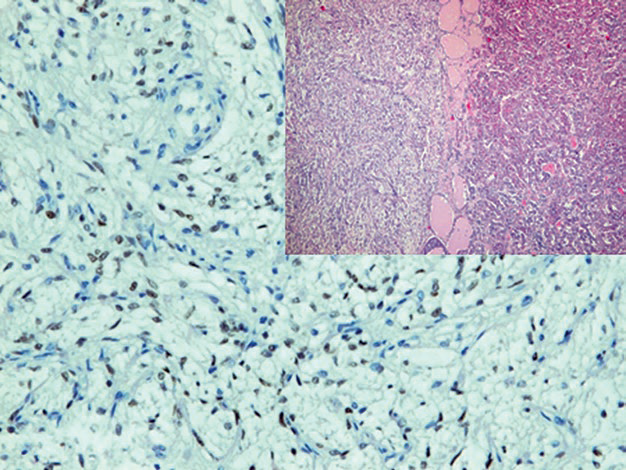
Figure 1. Cells in the neurohypophysis express TTF-1.
Overview of Immunohistochemical Indicators for Adrenal Tumor Diagnosis
The adrenal gland shares some similarities with the pituitary; for example, the pituitary is divided into adenohypophysis and neurohypophysis, while the adrenal gland can also be divided into cortex and medulla, and tumor types differ in different regions. However, some tumor types occurring outside the adrenal gland are similar to adrenal tumors, such as the correlation between extra-adrenal paraganglioma and adrenal pheochromocytoma, therefore they are also included in this chapter for study.
Table 3. Overview of Immunohistochemical Characteristics of Adrenal Tumors and Related Tumors
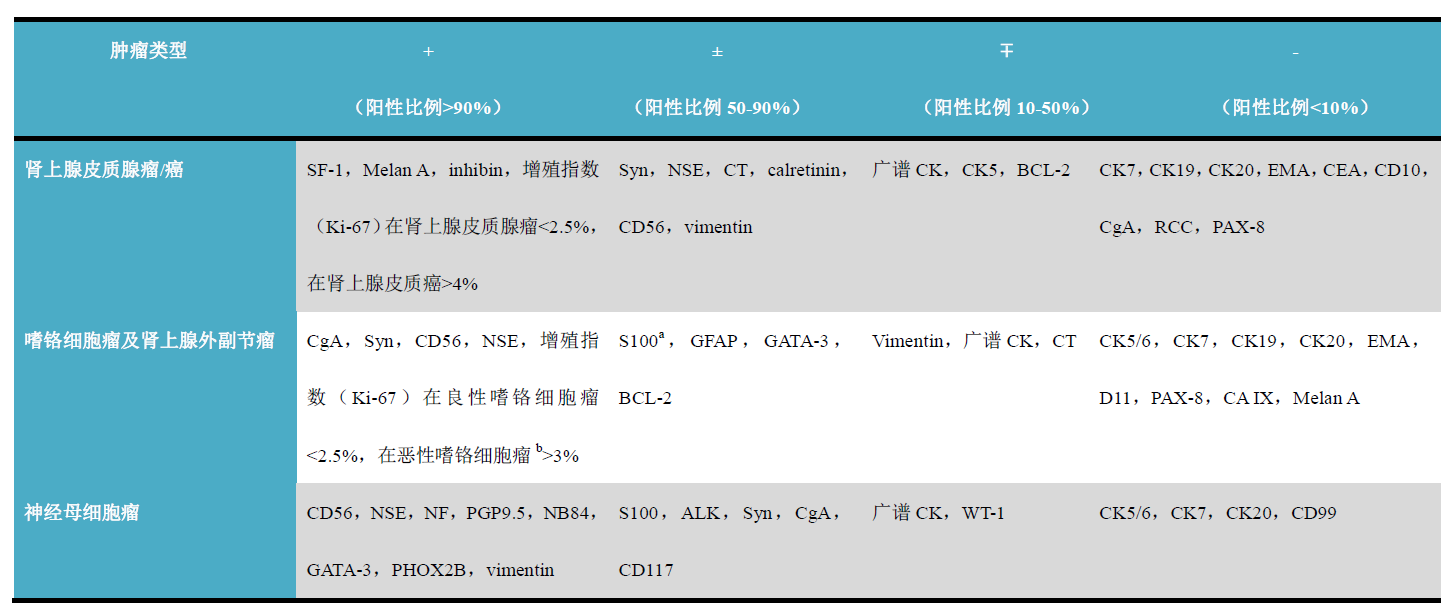
(Click to view larger image)
-
Strong nuclear positivity in sustentacular cells;
-
Malignant diagnosis cannot be definitively determined solely based on this criterion.
i. Adrenal Cortical Tumors
Commonly used immunohistochemical markers for diagnosis include: SF-1, DAX-1, inhibin, Melan A, calretinin, Syn, podoplanin, WT-1. Generally speaking, positivity for Syn, Melan A, inhibin, D2-40, calretinin along with co-expression of vimentin and CK5 supports an adrenal cortical origin of the tumor.
Detailed Explanation of Some Indicators
Positive expression pattern: Nucleus
Recommended positive control tissue: Adrenal gland
Steroid factor 1 (SF-1) belongs to the orphan nuclear receptor family and is a transcription factor regulating steroid hormone production. Normally, it is expressed in the adrenal cortex, pituitary gland, Sertoli cells, and various tumors derived from these cells. Renal cell carcinoma, hepatocellular carcinoma, malignant melanoma, and pheochromocytoma are consistently negative.
It should be noted that the diagnosis of metastatic adrenal cortical carcinoma must be combined with clinical and other relevant information, because sex cord-stromal tumors may be very similar to adrenal cortical tumors in morphology and immunohistochemistry.
Positive expression pattern: Cytoplasm
Recommended positive control tissue: Appendix
DAX-1 is also a member of the orphan nuclear receptor family; the function of this nuclear receptor protein is to inhibit the function of the aforementioned SF-1, thereby inhibiting steroid hormone production in the adrenal cortex. Additionally, DAX-1 plays a positive role in the development of the hypothalamic-pituitary-adrenal-gonadal axis and osteoblast differentiation.
DAX-1 expression is limited to steroid hormone-producing cells, such as related cells in the adrenal cortex, pituitary, hypothalamus, testis, ovary, etc. Similar to SF-1, DAX-1 is a marker for adrenal cortical tumors and certain tumors in the ovary, testis, and breast. It should be noted that,due to genetic abnormalities associated with Ewing sarcoma (EWS/Fli-1 translocation) promoting DAX-1 expression, this marker can also serve as a specific indicator for Ewing sarcoma.
This marker has been described in the previous chapter on sex cord tumors. Normally, inhibin is expressed in the gonads and adrenal glands, but the strongest expression in the adrenal gland is in the zona fasciculata and zona reticularis of the adrenal cortex; the adrenal medulla does not express it. Therefore, besides the aforementioned sex cord tumors of the testis and ovary, inhibin is also an important marker for benign and malignant adrenal cortical tumors.
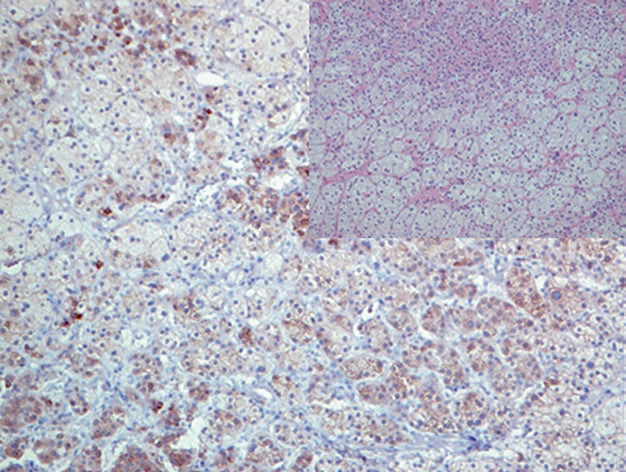
Figure 2. Adrenal cortical adenoma, inhibin positive in the cytoplasm.
ii. Adrenal Medullary Tumors, Neuroblastoma, and Extra-adrenal Paraganglioma
Commonly used immunohistochemical markers include: CgA, Syn, CD56, NSE, S100, GATA-3, most of which are detailed in other respective chapters; additionally, there are NB84, PGP9.5, CD117, NF, etc.
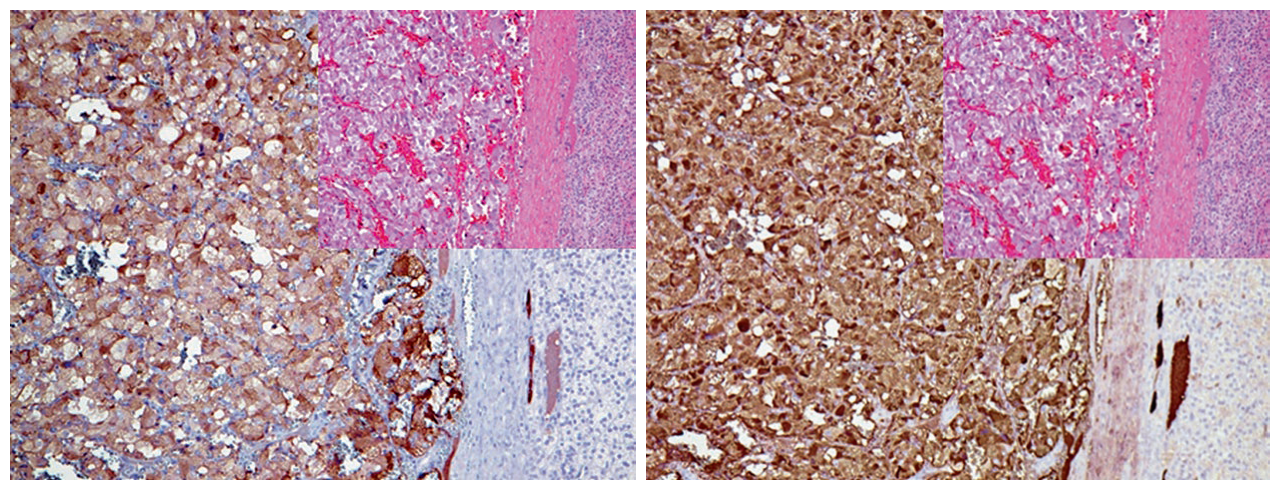
Figure 3. Pheochromocytoma, immunohistochemistry shows strong positive expression for CD56 (left) and Syn (right).
Detailed Explanation of Some Indicators
Positive expression pattern: Cell membrane
Recommended positive control tissue: Neuroblastoma
NB84 is a membrane antigen located on human neuroblastoma cells; the positive rate in immunohistochemistry is approximately 100% in differentiated neuroblastoma and about 90% in undifferentiated neuroblastoma. Compared to Syn, NB84 is more sensitive but less specific. For the diagnosis of adrenal and extra-adrenal related tumors, it is recommended to use three to four of the above markers in combination.
It should be noted that tumors morphologically similar to neuroblastoma can also show NB84 positivity, specifically such as PNET and desmoplastic small round cell tumor. To exclude these tumors, CD99 and CK should be included in the immunohistochemical detection panel. Also note the aforementioned point: a minority of undifferentiated neuroblastomas do not express NB84.
This series of articles has previously described this marker; it can be expressed in tumors of the breast, salivary glands, parathyroid, and urothelium. For the adrenal gland, GATA-3 is strongly positive in fetal sympathicoblasts, chromaffin cells in the adrenal medulla, and sympathetic paraganglia derived from sympathicoblasts; therefore, GATA-3 is a marker for adrenal medullary tumors and extra-adrenal paraganglioma tumors, such as pheochromocytoma and neuroblastoma.
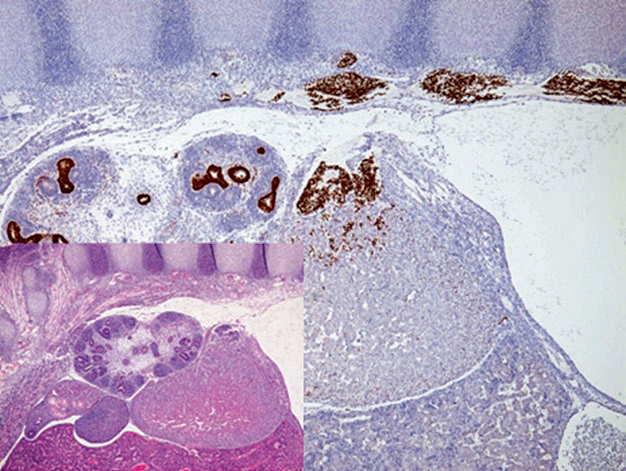
Figure 4. Tissue section of a 12-week embryo, immunohistochemistry with GATA-3 labeling sympathicoblasts in the paravertebral neural crest. These cells migrate into the dorsomedial aspect of the primitive adrenal gland to form the adrenal medulla; GATA-3 also labels urothelium in the renal collecting system.
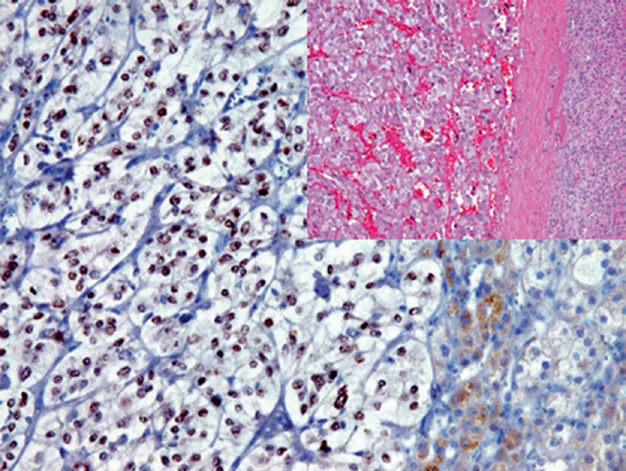
Figure 5. Pheochromocytoma, tumor cell nuclei express GATA-3.
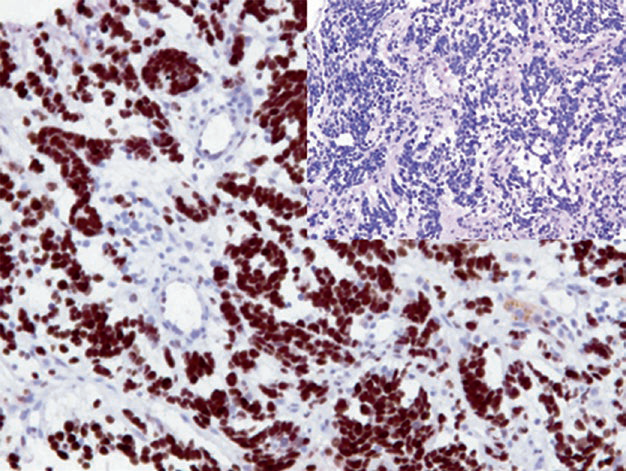
Figure 6. A case of adrenal biopsy, neuroblastoma cell nuclei express GATA-3.
It should be noted that adrenal cortex and adrenal cortical tumors can also show very low-level expression of GATA-3.
MaiMai Recommendation: “Based on morphology, selecting sufficient and reasonable immunohistochemical marker antibodies is of great value for the precise diagnosis of tumors as well as clinical treatment and prognosis assessment, but a ‘good antibody’ is the prerequisite and foundation for all of this.”
|
Antibody Name
|
Clone Number
|
Positive Control
|
Cellular Localization
|
|
GATA-3
|
L50-823
|
Urothelial carcinoma, Breast cancer
|
Nucleus
|
|
Inhibin α*
|
MX098
|
Ovarian granulosa cell tumor, Adrenal cortical adenoma
|
Cytoplasm
|
|
SF-1*
|
MX105
|
Pituitary adenoma, Testis |
Nucleus
|
*Marked as Maxin clone products
For more information, please inquire: 800-8581156 or 400-889-9853